This document summarizes pelvic anatomy, classification of pelvic ring injuries, and radiographic evaluation. It describes:
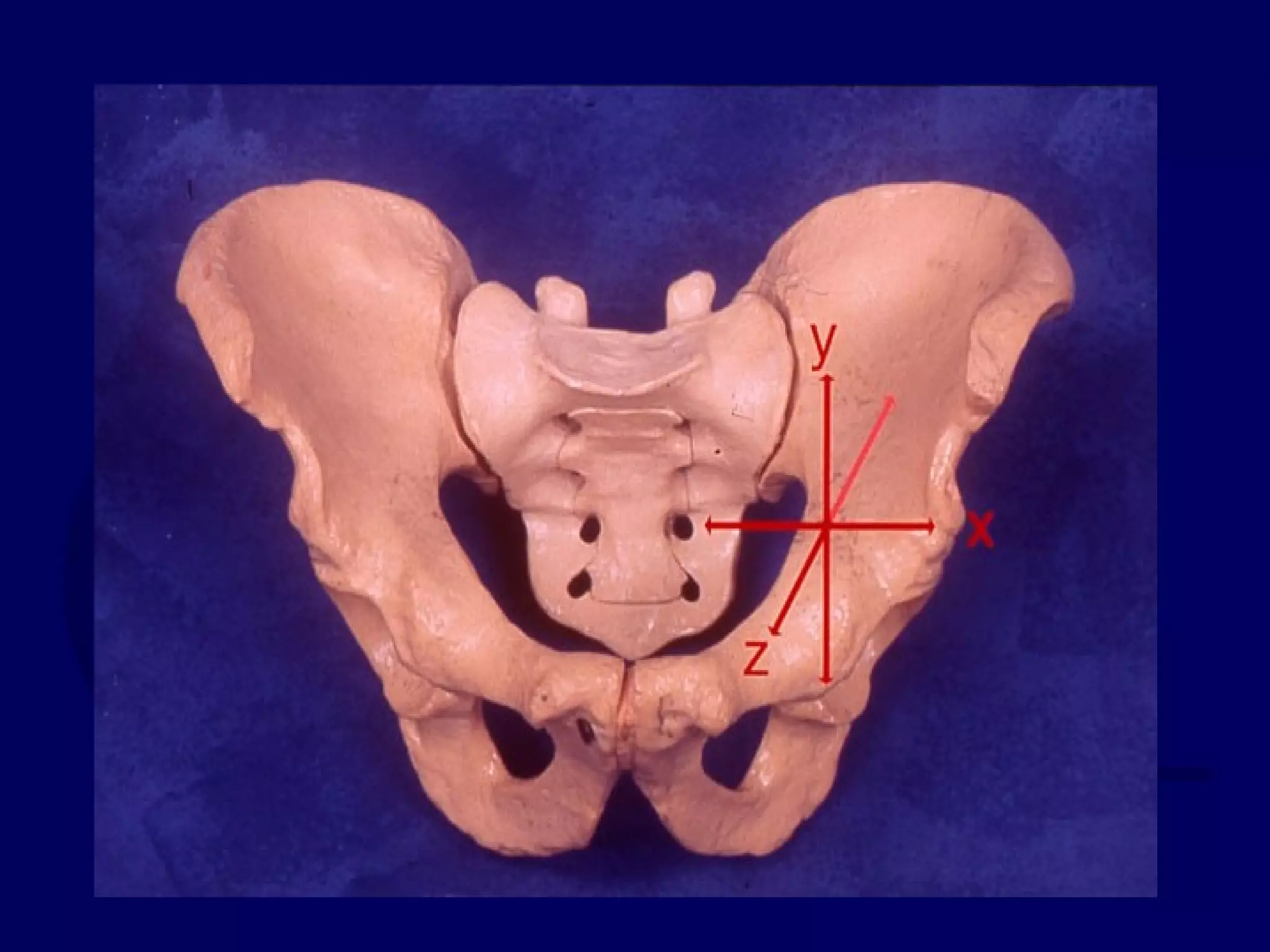
1) Important pelvic landmarks, ligaments, muscles, and arterial bleeders. Neurologic damage most commonly involves L5 and S1 nerves.
2) Classification systems include the anatomical Letournel system and the stability-focused systems of Pennal, Bucholz, and Tile.
3) The Young-Burgess system predicts associated injuries based on the vector force and classifies injuries as lateral compression, anteroposterior compression, or vertical shear.
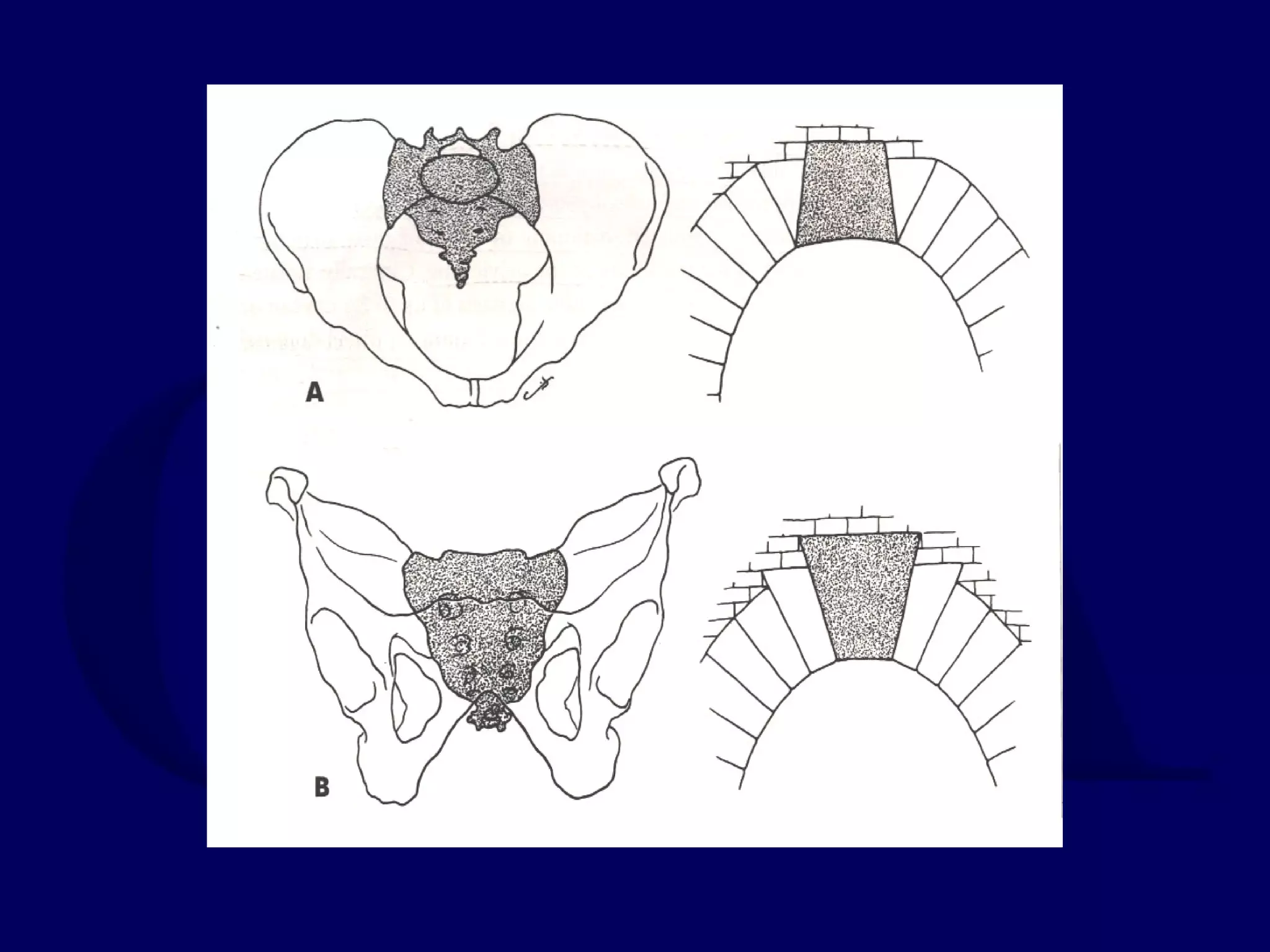
4) Radiographic evaluation involves anteroposterior, inlet, and outlet views on radiographs