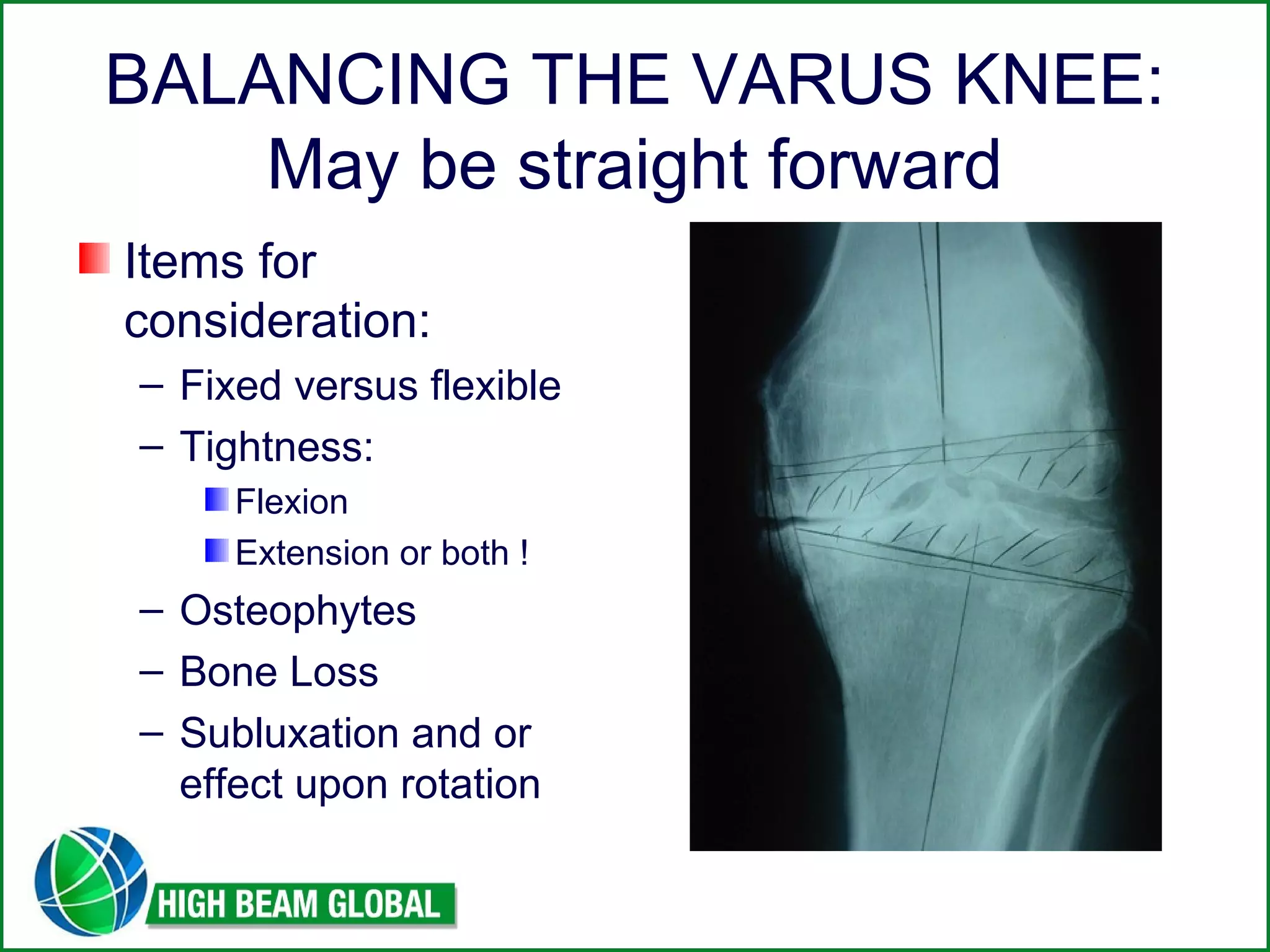
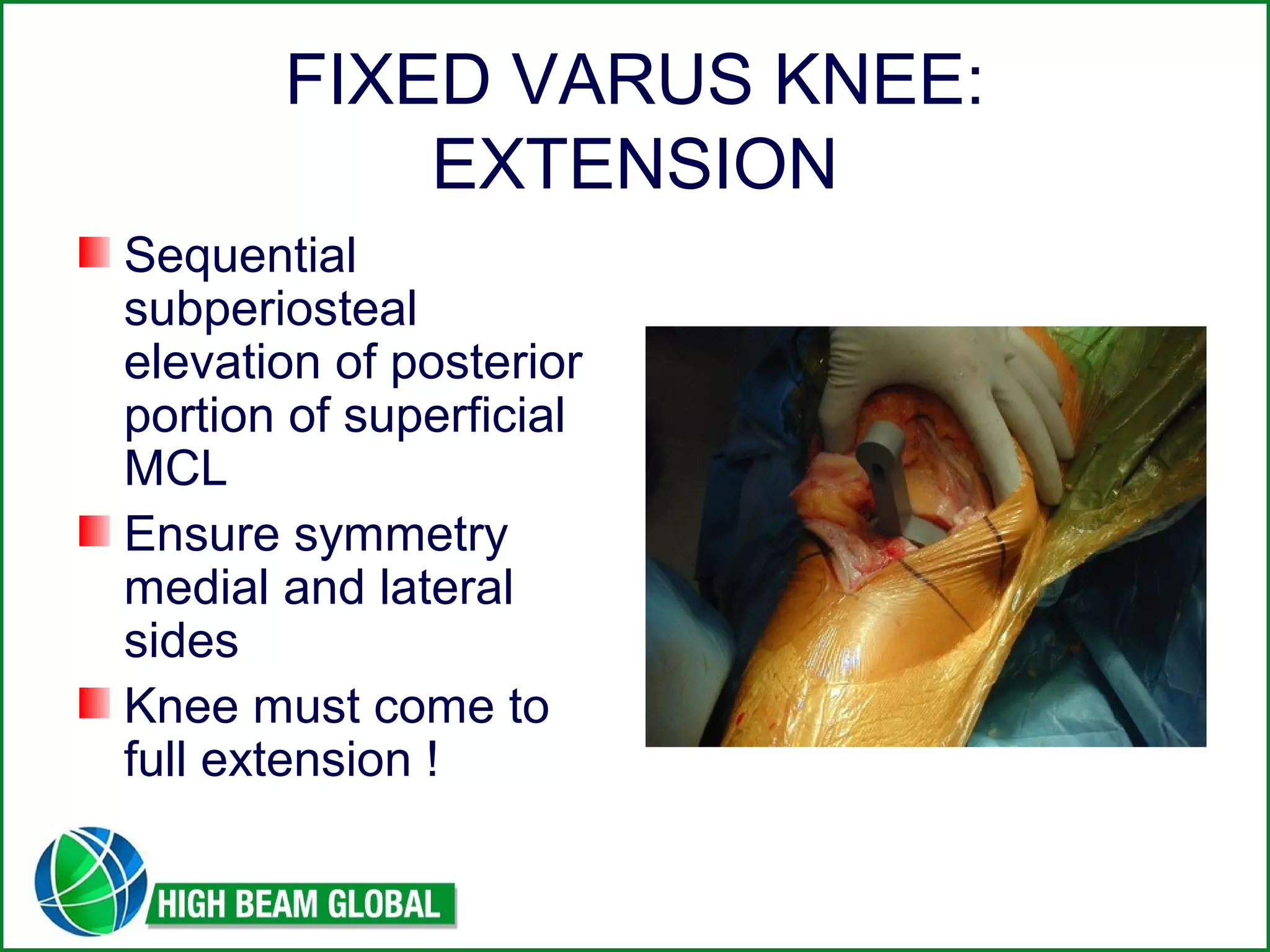
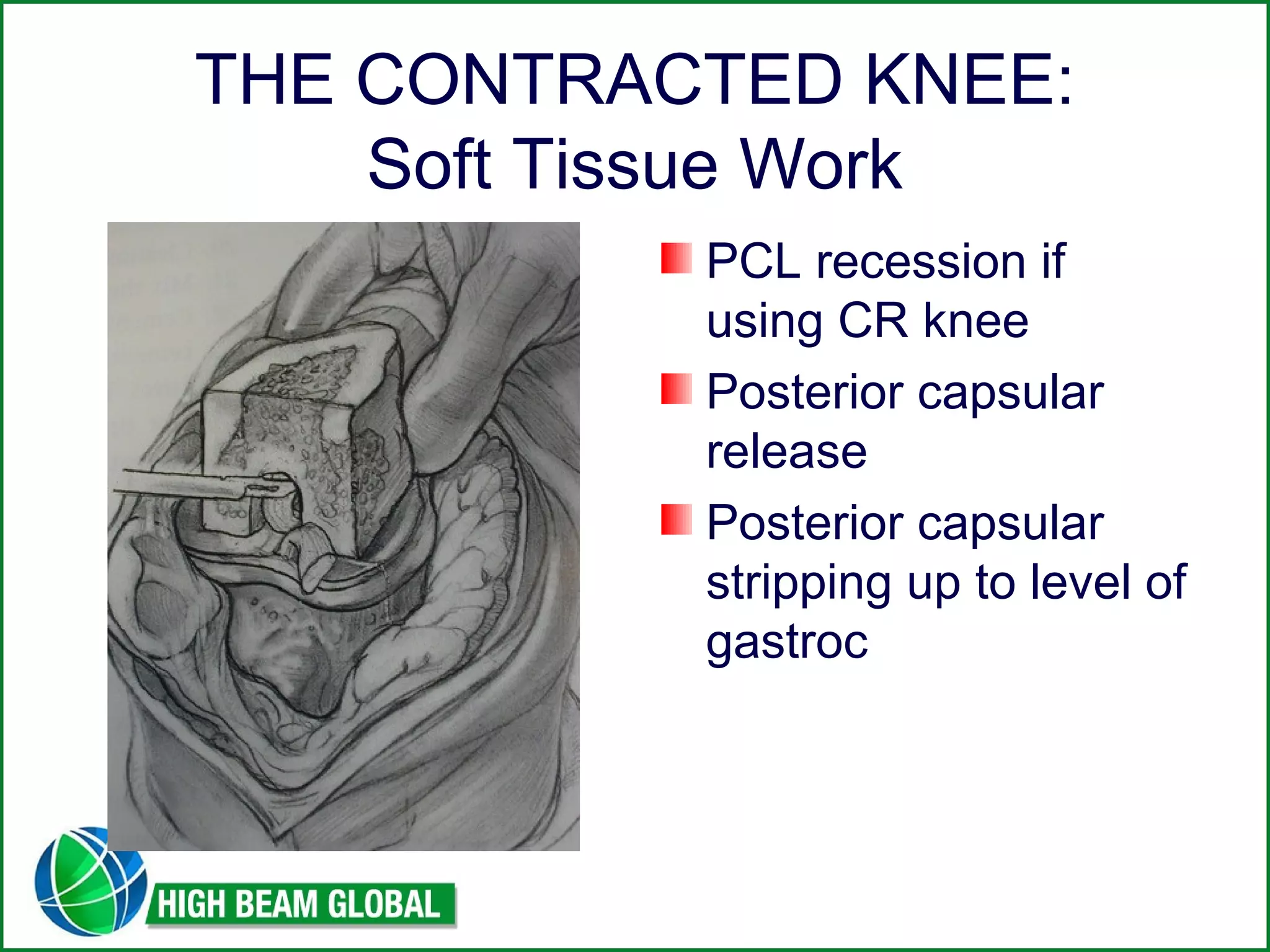
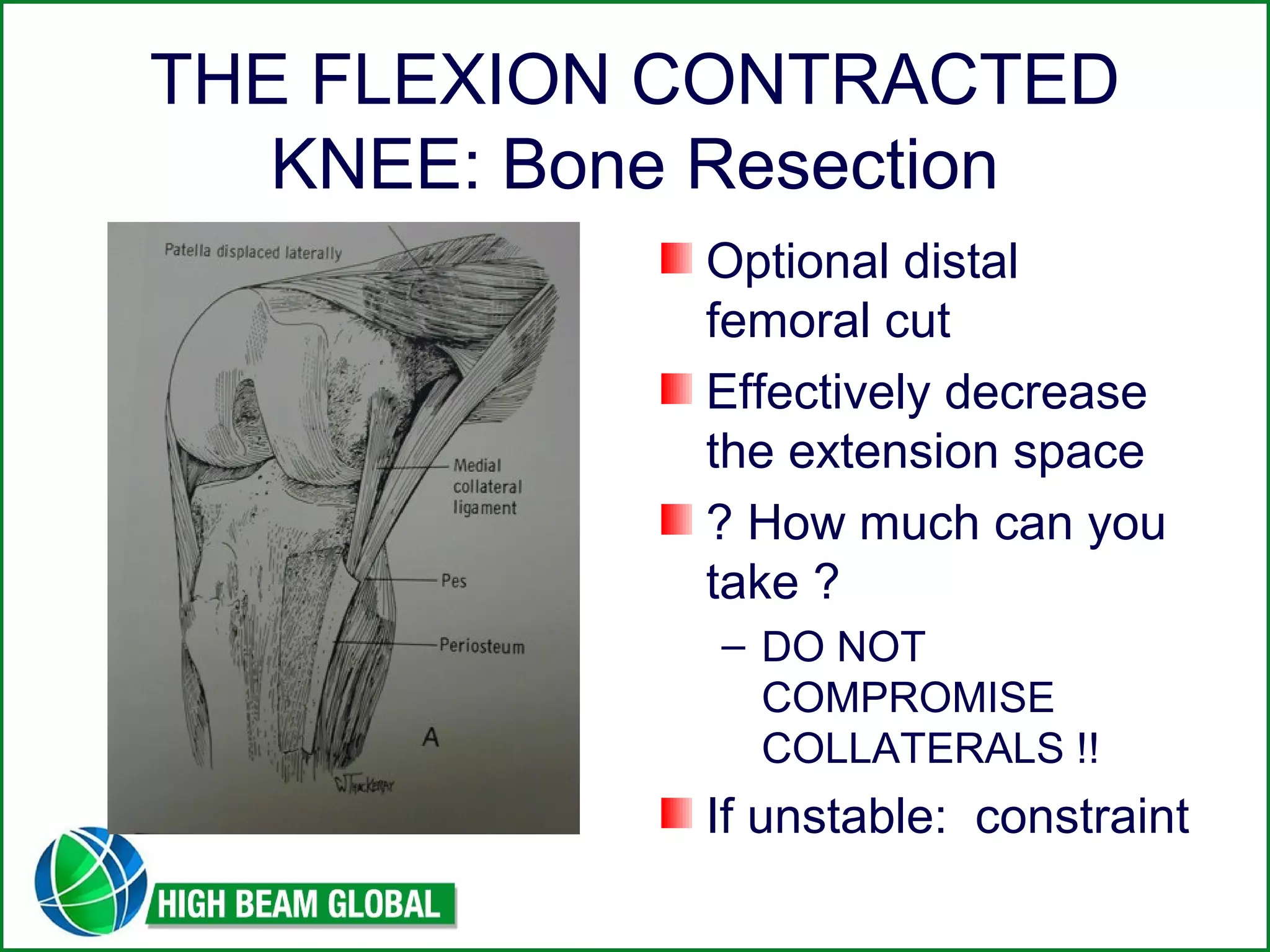
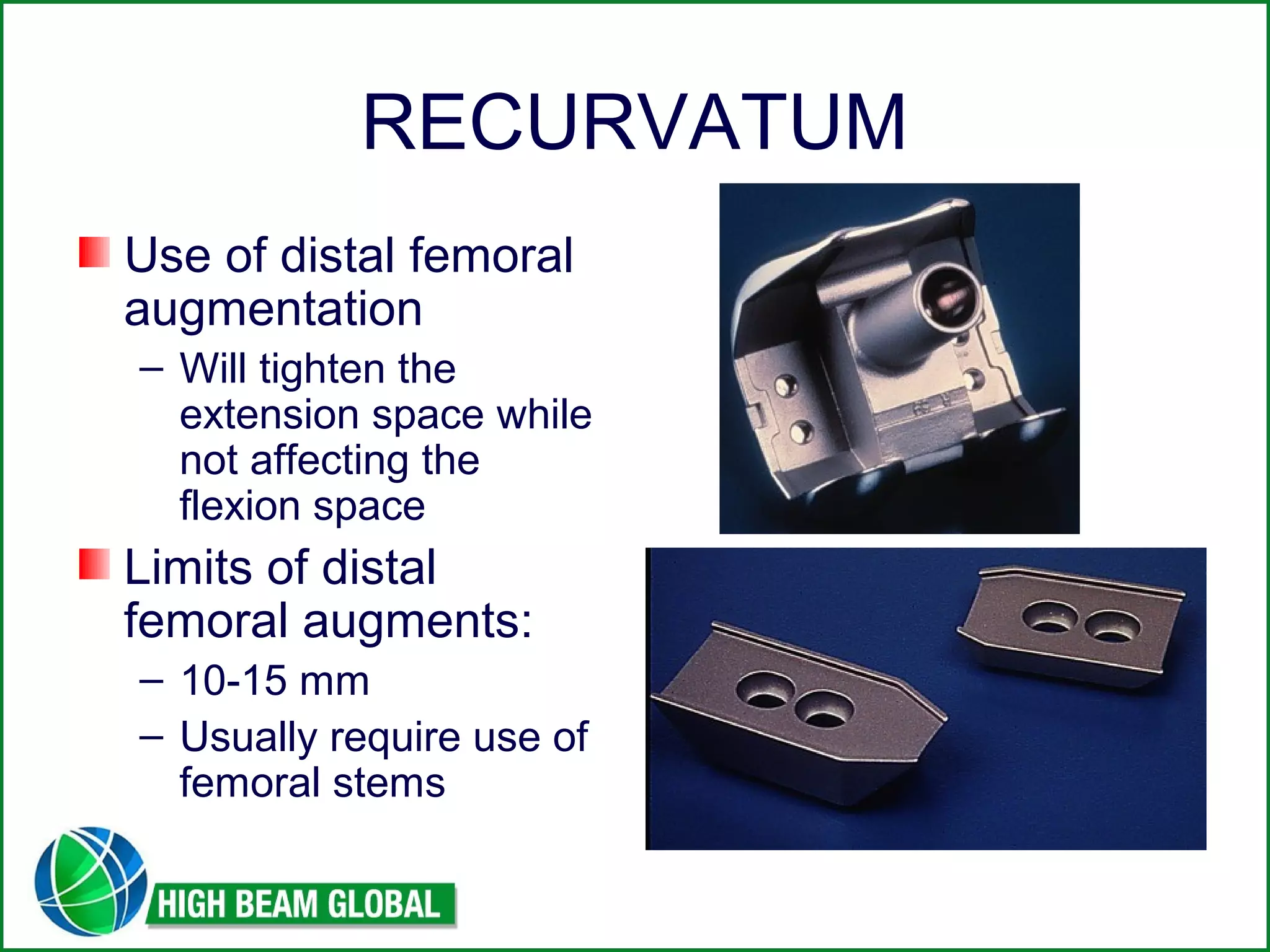
This document discusses techniques for balancing the soft tissues during primary total knee arthroplasty. It addresses approaches for correcting varus and valgus deformities, flexion contractures, and recurvatum. The key points emphasized are thoroughly assessing ligament balances and gaps, performing soft tissue releases in a sequential manner, and understanding how bone resections can impact soft tissue tension. Achieving balanced extension and flexion spaces between the medial and lateral sides is critical to surgical success.