Downloaded 66 times
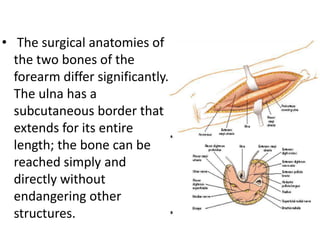
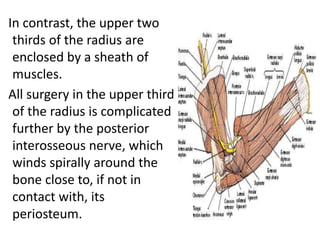
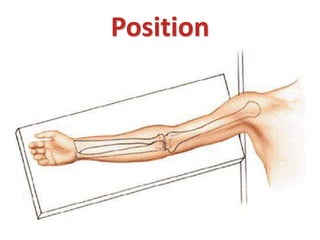
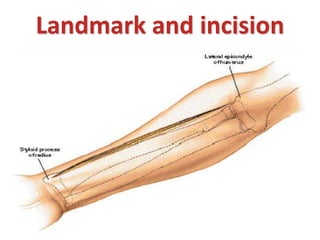
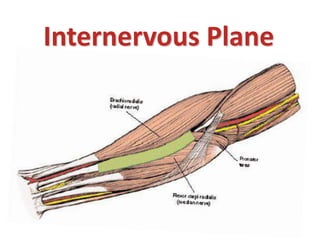
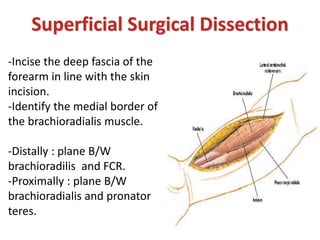
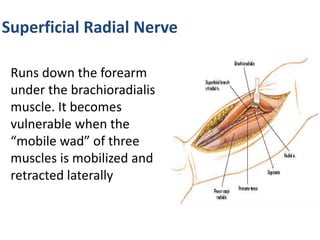
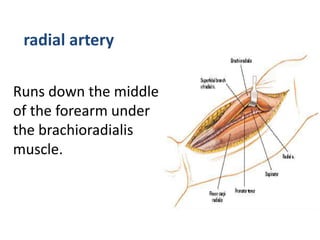

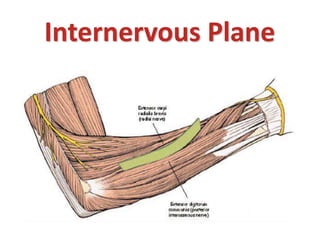



This document provides an overview of surgical approaches to the forearm bones - the radius and ulna. It describes the anterior and posterior approaches to the radius, including landmarks, incisions, planes of dissection, and dangers such as the posterior interosseous nerve. The approach to the ulna is also outlined. The goal is to expose the bones while protecting surrounding nerves and muscles through careful subperiosteal dissection in appropriate intermuscular planes.























































































