Downloaded 776 times
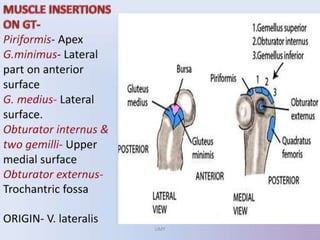
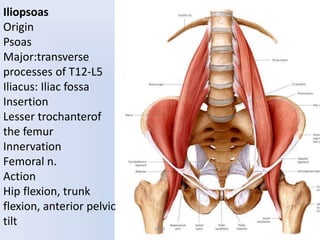

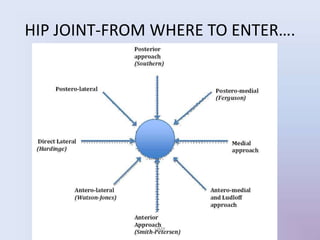
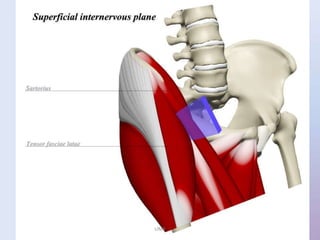
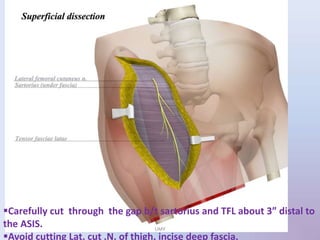
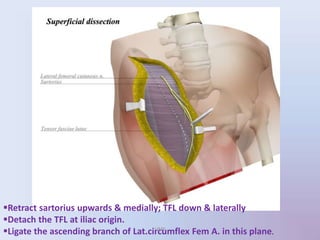
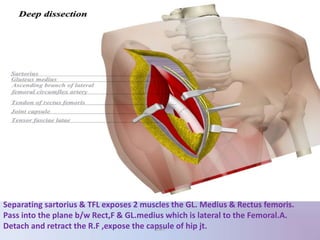
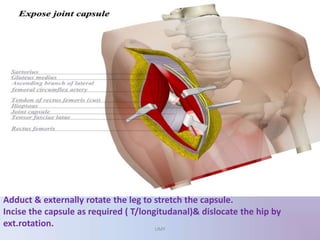
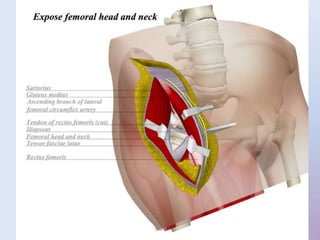
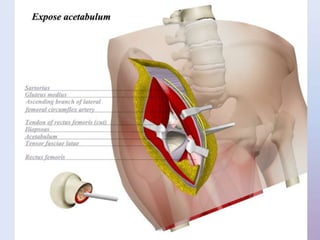
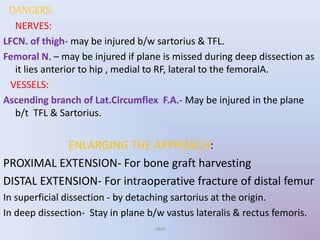
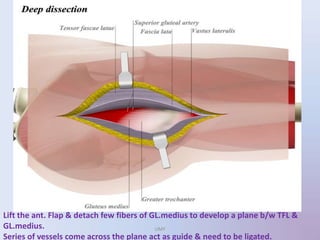
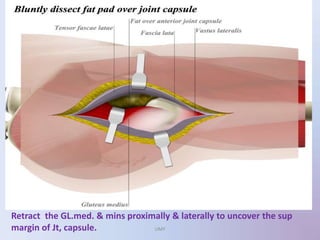
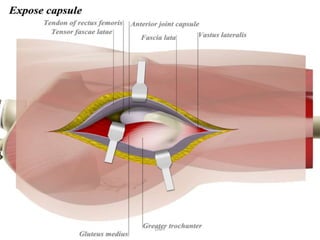
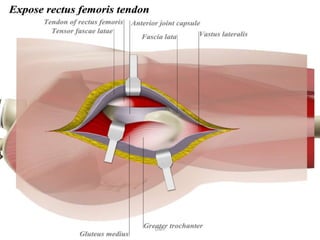
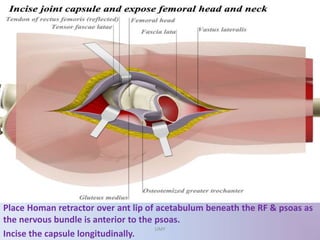
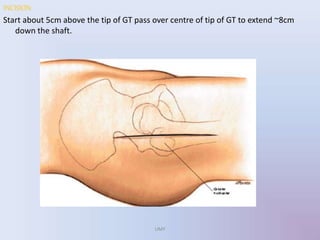
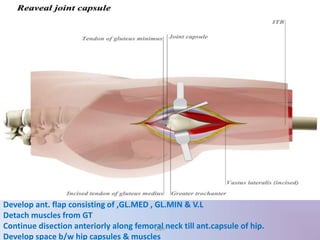
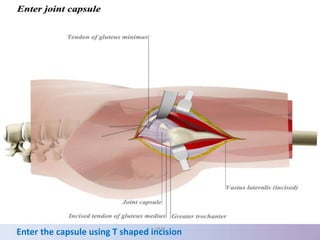
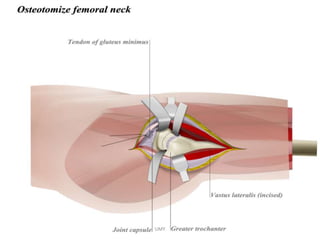
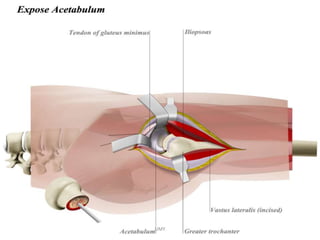

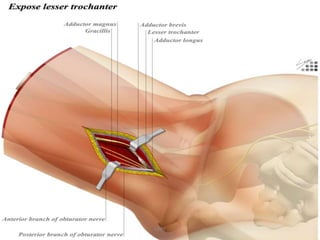

1) The document provides an overview of the anatomy related to the hip joint and surgical approaches to the hip joint including the anterior (Smith Peterson) approach, anterolateral (Watson Jones) approach, and lateral approach. 2) Key muscles and nerves are identified along with their origins, insertions, innervation and actions. 3) Each surgical approach is described in terms of indications, landmarks, incision, internervous planes, steps of the procedure and potential dangers. Maintaining the correct internervous planes is important to avoid injury to nerves and vessels.































































































