Downloaded 174 times




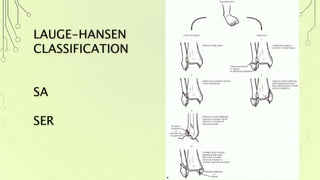

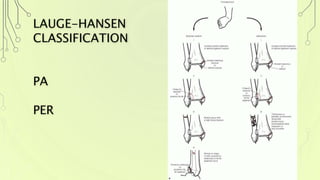


This document discusses ankle fractures and the Lauge-Hansen classification system. The Lauge-Hansen system categorizes ankle fractures based on the position of the foot and direction of force at the time of injury. The four main categories are supination-adduction, supination-external rotation, pronation-abduction, and pronation-external rotation. Each category represents a different mechanism of injury and has characteristics regarding the order and nature of bone and ligament injuries. The classification system provides a standardized way to describe ankle fractures based on their mechanism of injury.















































































