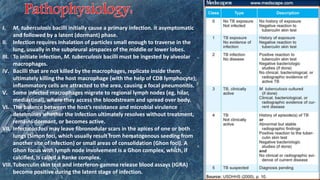
Tuberculosis (TB) is a chronic infection primarily affecting the lungs and is a leading cause of morbidity and mortality globally, especially in low-income regions. It can be classified as open or closed, pulmonary or extrapulmonary, and transmission occurs mainly through airborne droplets from infected individuals. Treatment typically involves a combination of first-line drugs and, if necessary, second-line medications, with appropriate therapy usually curative for drug-susceptible cases.