Tuberculosis
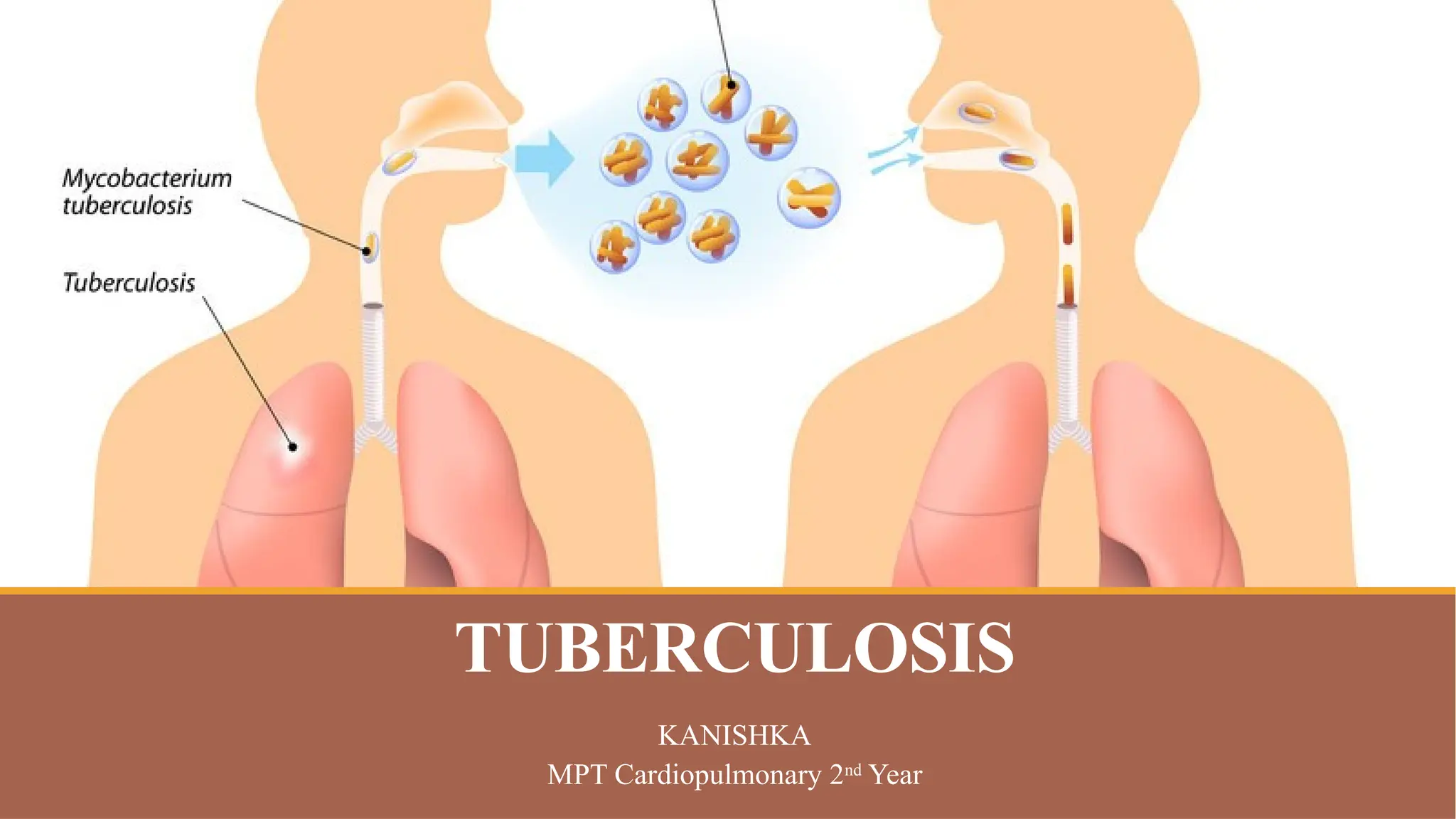
Tuberculosis (TB) isa bacterial disease caused by Mycobacterium tuberculosis.
It is a highly contagious disease and is currently the leading cause of death from a
single infectious pathogen.
TB is a multi-systemic disease. It mainly affects the lungs, making pulmonary
disease the most common presentation.
Other commonly affected organ systems include the respiratory system, the
gastrointestinal (GI) system, the lymphoreticular system, the skin, the central
nervous system, the musculoskeletal system, the reproductive system, and the
liver.
It is a serious condition, but can be cured with proper treatment.
3.
Epidemiology
In the pastfew decades, there has been a concerted global effort to eradicate TB.
These efforts had yielded some positive results, especially since 2000 when the
World Health Organization (2017) estimated that the global incidence rate for
tuberculosis has fallen by 1.5% every year.
Furthermore, mortality arising from tuberculosis has significantly and steadily
declined. The World Health Organization (2016) reports a 22% drop in global
TB mortality from 2000 through 2015.
The bulk of the global burden of new infection and tuberculosis death is borne
by developing countries, with 6 countries, India, Indonesia, China, Nigeria,
Pakistan, and South Africa, accounting for 60% of TB death in 2015.
4.
Etiology
TB is causedby Mycobacterium tuberculosis.
M. tuberculosis is an alcohol and acid-fast bacillus.
It is part of a group of organisms classified as the M. tuberculosis complex.
Other members of this group are Mycobacterium africanum, Mycobacterium
bovis, and Mycobacterium microti. Most other mycobacteria organisms are
classified as non-tuberculous or atypical mycobacterial organisms.
M. tuberculosis is a non-spore-forming, non-motile, obligate-aerobic,
facultative, catalase-negative, intracellular bacteria.
The organism is neither gram-positive nor gram-negative because of a very poor
reaction with the Gram stain. The Ziehl-Neelsen stain is one of the most
commonly used stains to diagnose TB.
5.
The organism hasseveral unique features compared to other bacteria, such as the
presence of several lipids in the cell wall, including mycolic acid, cord factor,
and Wax-D. The high lipid content of the cell wall is thought to contribute to the
following properties of M. tuberculosis infection:
Resistance to several antibiotics
Difficulty staining with Gram stain and several other stains
Ability to survive under extreme conditions such as extreme acidity or
alkalinity, low oxygen situation, and intracellular survival(within the
macrophage)
6.
Major Risk Factors
Socioeconomicfactors: Poverty, malnutrition, wars
Immunosuppression: HIV/AIDS, chronic immunosuppressive therapy (steroids,
monoclonal antibodies against tumor necrotic factor), a poorly developed
immune system (children, primary immunodeficiency disorders)
Occupational: Mining, construction workers, pneumoconiosis (silicosis)
7.
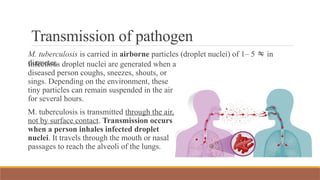
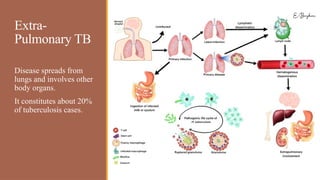
Transmission of pathogen
M.tuberculosis is carried in airborne particles (droplet nuclei) of 1– 5 in
diameter.
Infectious droplet nuclei are generated when a
diseased person coughs, sneezes, shouts, or
sings. Depending on the environment, these
tiny particles can remain suspended in the air
for several hours.
M. tuberculosis is transmitted through the air,
not by surface contact. Transmission occurs
when a person inhales infected droplet
nuclei. It travels through the mouth or nasal
passages to reach the alveoli of the lungs.
8.
Pulmonary TB Primarytuberculosis: The infection of an
individual who has not been previously infected or
immunised is called Primary tuberculosis.
Lesions forming after infection is peripheral and
accompanied by hilar which may not be detectable
on chest radiography.
Secondary tuberculosis: The infection that
individual who has been previously infected or
sensitized is called Secondary or post primary or
chronic tuberculosis.
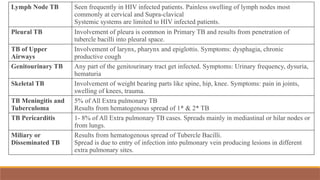
Lymph Node TBSeen frequently in HIV infected patients. Painless swelling of lymph nodes most
commonly at cervical and Supra-clavical
Systemic systems are limited to HIV infected patients.
Pleural TB Involvement of pleura is common in Primary TB and results from penetration of
tubercle bacilli into pleural space.
TB of Upper
Airways
Involvement of larynx, pharynx and epiglottis. Symptoms: dysphagia, chronic
productive cough
Genitourinary TB Any part of the genitourinary tract get infected. Symptoms: Urinary frequency, dysuria,
hematuria
Skeletal TB Involvement of weight bearing parts like spine, hip, knee. Symptoms: pain in joints,
swelling of knees, trauma.
TB Meningitis and
Tuberculoma
5% of All Extra pulmonary TB
Results from hematogenous spread of 1* & 2* TB
TB Pericarditis 1- 8% of All Extra pulmonary TB cases. Spreads mainly in mediastinal or hilar nodes or
from lungs.
Miliary or
Disseminated TB
Results from hematogenous spread of Tubercle Bacilli.
Spread is due to entry of infection into pulmonary vein producing lesions in different
extra pulmonary sites.
11.
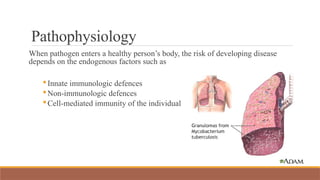
Pathophysiology
When pathogen entersa healthy person’s body, the risk of developing disease
depends on the endogenous factors such as
Innate immunologic defences
Non-immunologic defences
Cell-mediated immunity of the individual
12.
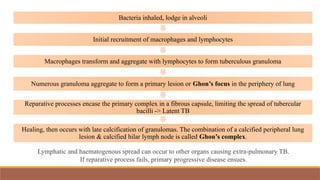
Bacteria inhaled, lodgein alveoli
Initial recruitment of macrophages and lymphocytes
Macrophages transform and aggregate with lymphocytes to form tuberculous granuloma
Numerous granuloma aggregate to form a primary lesion or Ghon’s focus in the periphery of lung
Reparative processes encase the primary complex in a fibrous capsule, limiting the spread of tubercular
bacilli -> Latent TB
Healing, then occurs with late calcification of granulomas. The combination of a calcified peripheral lung
lesion & calcified hilar lymph node is called Ghon’s complex.
Lymphatic and haematogenous spread can occur to other organs causing extra-pulmonary TB.
If reparative process fails, primary progressive disease ensues.
13.
1. Following M.
tuberculosisinfection,
the bacilli reach the
lungs.
2. They provoke a host
immune response.
3. This in turn leads to
granuloma formation.
4. (a) The granuloma
contains the bactria and
typically suppresses the
infection in its latent
state.
(b) However,
reactivation can occur,
resulting in an active
disease state in which
the disease can spread to
other individuals.
14.
Clinical Presentation
Clinical symptomsof active tuberculosis (TB) can range from a simple cough to
more severe reactions, such as irreversible lung damage and, eventually, death,
depending on disease progression.
General Symptoms Pulmonary Symptoms Extra Pulmonary Symptoms
Weight loss
Extreme tiredness or
Fatigue
Night sweats
Low grade fever
Anorexia
Chest pain, Dyspnea
Persistent cough that lasts more
than three weeks and usually
brings up phlegm, which may be
bloody
Non-productive cough
Chest tightness
Non-resolving bronchopneumonia
Inflammation
Pain
Organ-specific symptoms
15.
Primary Pulmonary TB
Vastmajority are asymptomatic. A few patients develop a self-limiting febrile illness.
Patient presents with:
Influenza like illness lasting for 7-14 days
Reduced weight and failure to gain weight.
Child is thin, pale and fretful with less elastic skin and less glossy hair.
Sometimes, crepitations may be heard in lung (at the site of primary complex)
Fever, arthralgia, erythema nodosum
Signs and symptoms may result from progression or complications of primary
complex.
16.
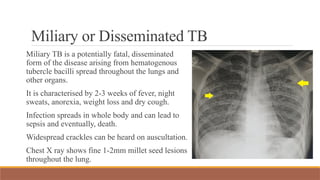
Miliary or DisseminatedTB
Miliary TB is a potentially fatal, disseminated
form of the disease arising from hematogenous
tubercle bacilli spread throughout the lungs and
other organs.
It is characterised by 2-3 weeks of fever, night
sweats, anorexia, weight loss and dry cough.
Infection spreads in whole body and can lead to
sepsis and eventually, death.
Widespread crackles can be heard on auscultation.
Chest X ray shows fine 1-2mm millet seed lesions
throughout the lung.
17.
Post-primary Pulmonary TB
GeneralSymptoms:
Loss of weight, loss of appetite
Fever, esp. evening rise of
temperature
Night sweats
Tiredness, malaise
Mental symptoms
Amenorrhoea
Respiratory Symptoms:
Cough (>3 wks of cough -> check for TB)
Sputum (mucoid, purulent, blood-stained)
Haemoptysis – classical symptom
Chest pain (pleurisy, intercostal myalgia, cough fracture)
Breathlessness in advanced & extensive disease
Localised wheeze due to narrowing of major bronchus
Recurrent URTI
Pneumonia which turns out to be TB
18.
Physical Signs
Pallor andcachexia
Fever, tachycardia and tachypnoea
Finger clubbing may be +nt in chronic
disease with purulent sputum
Percussion: dullness over area or
consolidation
Auscultation: bronchial breath sounds and
fine crepts in upper part of lung; localised
wheezing due to narrowing of bronchus
19.
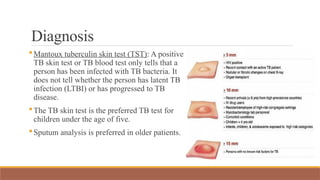
Diagnosis
Mantoux tuberculin skintest (TST): A positive
TB skin test or TB blood test only tells that a
person has been infected with TB bacteria. It
does not tell whether the person has latent TB
infection (LTBI) or has progressed to TB
disease.
The TB skin test is the preferred TB test for
children under the age of five.
Sputum analysis is preferred in older patients.
20.
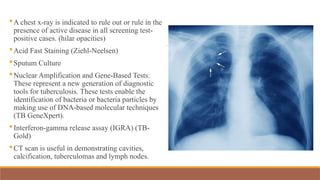
A chest x-rayis indicated to rule out or rule in the
presence of active disease in all screening test-
positive cases. (hilar opacities)
Acid Fast Staining (Ziehl-Neelsen)
Sputum Culture
Nuclear Amplification and Gene-Based Tests:
These represent a new generation of diagnostic
tools for tuberculosis. These tests enable the
identification of bacteria or bacteria particles by
making use of DNA-based molecular techniques
(TB GeneXpert).
Interferon-gamma release assay (IGRA) (TB-
Gold)
CT scan is useful in demonstrating cavities,
calcification, tuberculomas and lymph nodes.
21.
Differential Diagnosis
The differentialdiagnosis can be broad, especially with respiratory involvement, but
can include the following:
Sarcoidosis: Mainly differentiated from TB by the presence of non-caseating
granuloma.
Fungal infections: Such as Aspergillosis, Actinomycosis, Blastomycosis.
Epidemiological history aid in determining the risk of developing these infections.
Nontuberculous mycobacterial infections (NTM): such as Mycobacterium kansasii.
Lung malignancy and lymphoma: Tissue biopsy is needed to rule out this diagnosis
if suspected
Lung abscess
22.
Complications
Bleeding from bronchial,pulmonary, and intercostal arteries lead to hemoptysis.
This bleeding is usually minimal and rarely leads to massive blood loss.
Rupture of a subpleural focus or a lung cavity could lead to spontaneous
pneumothorax.
Lymph node inflammation may lead to compression on the bronchial tree and
could cause bronchiectasis.
Severe untreated pulmonary TB may lead to extensive lung destruction, necrosis,
and gangrene.
Tuberculosis has also been reported to increase the risk of lung malignancy.
Secondary metabolic complications such as glucose intolerance and vitamin D
deficiency, etc.
23.
Treatment and Management
Themost effective approach for tuberculosis disease prevention is identifying
cases and effective treatment.
Medical therapy considerably decreases bacterial load transmission within
communities.
BCG vaccine is usually given at birth or in infancy (upto 6 months), particularly in
developing countries. The vaccine seems to decrease the incidence of tuberculosis
in childhood but unfortunately does not affect the incidence of adulthood disease.
Contagiousness decreases rapidly once effective treatment begins; cough decreases,
and organisms are noninfectious even if they persist in sputum. Studies suggest that
transmission ends within a few days to 2 weeks of starting treatment.
24.
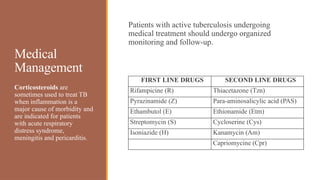
Medical
Management
Patients with activetuberculosis undergoing
medical treatment should undergo organized
monitoring and follow-up.
Corticosteroids are
sometimes used to treat TB
when inflammation is a
major cause of morbidity and
are indicated for patients
with acute respiratory
distress syndrome,
meningitis and pericarditis.
FIRST LINE DRUGS SECOND LINE DRUGS
Rifampicine (R) Thiacetazone (Tzn)
Pyrazinamide (Z) Para-aminosalicylic acid (PAS)
Ethambutol (E) Ethionamide (Etm)
Streptomycin (S) Cycloserine (Cys)
Isoniazide (H) Kanamycin (Am)
Capriomycine (Cpr)
25.
DOTS – DirectlyObserved Treatment
Short Course
Tuberculosis control strategy recommended by the WHO as the strategy that
ensures cure of TB.
Directly observed treatment (DOT) is one element of the DOTS strategy
An observer watches and helps the patient swallow the tablets
Direct observation ensures treatment for the entire course
With the right drugs
In the right doses
At the right intervals
26.
There are twophases in DOTS treatment.
Intensive Phase: Intensive phase is of 2 to 3 months.
◦ Patient swallow medicine under the observation of a health worker during IP.
◦ .Medicines are taken 3 times a week on alternate days.
◦ If the sputum is negative for bacteria after IP, continuation phase is started.
Continuation Phase: This phase is of 4 or 5 months duration.
◦ The patient is provided with a weekly blister pack to take home.
◦ The medicines from the blister pack are taken on alternate days, 3x week and
on the remaining days, vitamin tablets are taken.
◦ The first dose of the weekly blister pack is taken under direct observation of
the health worker.
◦ Empty blister packs are collected to ensure that the medicines are taken at
home by the patient.
27.
Drug-resistant Tuberculosis
Drug resistanceis a major problem in treating tuberculosis. It is a major
challenge that could arise during treatment. The chance of developing MDR TB
is around 3.8% in developed countries. However, this number could be much
higher in countries with a high TB burden, such as China and India, reaching up
to 20%. Drug-resistant TB is categorized into different types:
◦ Mono-resistant TB: Resistance to one of the drugs of standard first-line
medications.
◦ Polydrug resistance: Resistance to more than one first-line medication (except
the combination of INH and RIF).
◦ Multidrug resistance (MDR): Resistance to both INH and RIF
◦ Extensive drug resistance (XDR): MDR plus resistance to a fluoroquinolone
and injectable second-line medications.
28.
Physiotherapy Management
People withactive pulmonary TB are typically not treated in physical therapy because
medications are vital for curing TB.
Percussion and postural drainage can be used to clear secretions out of the lung.
Breathing exercises can be taught to reduce work of breathing and relieve dyspnoea.
Individuals with TB of spine and joints may require physiotherapy treatment for pain reief and
mobility.
29.
Recent evidence showeffectiveness of PR program in individuals with post TB sequelae.
A comprehensive 3-week PR programme was devised including:
Specialist nurse training (inhalation techniques and/or oxygen-therapy when prescribed);
18 aerobic-training sessions by cycle ergometer supervised by a respiratory therapist
5 sessions/wk, 30 min each: 5 min warm-up, 20 min training and 5 min warm-down) at
constant load.
Optional PR components included: inspiratory muscle conditioning , breathing exercises,
airways clearance, psychological support (3 sessions/wk), relaxation (5 sessions/wk) and
nutritional counselling (personalised diet).
Patients attended two educational group sessions, managed by a respiratory therapist, on
lifestyle, physical activity and maintenance programmes.
Subjects with impaired lung function showed a significant improvement in 6-min
walking distance, in final Borg dyspnoea and fatigue scores, as well as of FEV1.
Data suggest that PR is effective in patients with a previous history of TB and with
lung function impairment.
30.
REFERENCES
Adigun, R.(2023, July 11). Tuberculosis. StatPearls - NCBI Bookshelf. https://
www.ncbi.nlm.nih.gov/books/NBK441916/
Heemskerk, D. (2015). Pathogenesis. Tuberculosis in Adults and Children - NCBI Bookshelf.
https://www.ncbi.nlm.nih.gov/books/NBK344406/
Luies L, du Preez I.2020.The Echo of Pulmonary Tuberculosis: Mechanisms of Clinical
Symptoms and Other Disease-Induced Systemic Complications. Clin Microbiol Rev
33:10.1128/cmr.00036-20. https://doi.org/10.1128/cmr.00036-20





















![Physiotherapy in pulmonary_surgery[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/pulmonarysurgery1-230705093621-2b78f958-thumbnail.jpg?width=640&height=640&fit=bounds)















































