Downloaded 592 times
![BLAMED
Baltimore-Washington Infant Study: maternal cigarette smoke(odds ratio [OR]: 1.9,
95% CI 1.04-3.45)
Texas Birth Defects Registry (1999 to 2004): advancing maternal age
22q11.2 deletions: Deletions in three genes in this locus (TBX1, CRKL, and ERK2)
cause neural crest cell and anterior heart anomalies seen in patients with DiGeorge
syndrome
Retinoic acid
Bismuth](https://image.slidesharecdn.com/truncusarteriosus-140205113055-phpapp01/85/Truncus-arteriosus-5-320.jpg)
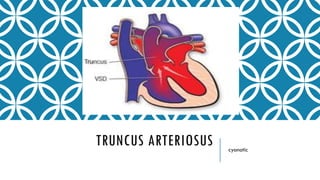
![EMBRYOLOGY
Defect in the development of the truncoconal[more conal than Truncus] septum result
in Conotruncal abnormalities including Truncus arteriosus
Neural crest hypothesis
Bulbar septum is deficient just below the singular truncal=semilunar valve](https://image.slidesharecdn.com/truncusarteriosus-140205113055-phpapp01/85/Truncus-arteriosus-6-320.jpg)

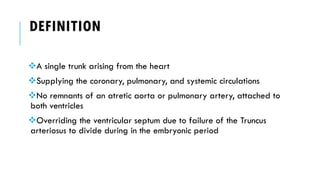
![VSD OR NO VSD[SOCIETY OF THORACIC
SURGEONS (STS) ]
TYPE A[VSD+] TYPE B[VSD-]
A1: As CE type 1, in which a main pulmonary artery is present, and
arises from the left side of the truncal root.
A2: h CE types II and III, as the two CE types do not differ
embryologically and the surgical approach is the same. Type A2
consists of right and left branch pulmonary arteries with separate
origins (regardless of the distance separating the two pulmonary
arteries) from the truncal root.
A3: Unilateral pulmonary atresia with collateral supply to the
affected lung.
A4:Interrupted aortic arch
Van Praagh R, Van Praagh S. The anatomy of common aorticopulmonary trunk (truncus arteriosus communis) and its
embryologic implications: a study of 57 necropsy cases. Am J Cariol 1965;16:406-26](https://image.slidesharecdn.com/truncusarteriosus-140205113055-phpapp01/85/Truncus-arteriosus-11-320.jpg)
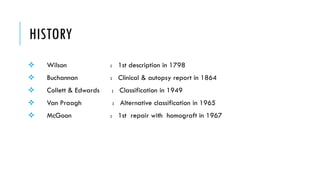
![Major classification systems for truncus arteriosus reproduced from [25] with permission from
Elsevier.
Sojak V et al. MMCTS 2012;2012:mms011
© The Author 2012. Published by Oxford University Press on behalf of the European Association
for Cardio-thoracic Surgery. All rights reserved](https://image.slidesharecdn.com/truncusarteriosus-140205113055-phpapp01/85/Truncus-arteriosus-12-320.jpg)
![TREATMENT
Initial medical management Surgery
Treat heart failure due to large left to right shunt Connect pulmonary artery[right ventricle to
pulmonary artery (RV-PA) conduits ] to right
ventricle
Primary surgical repair during the neonatal period
(less than 30 days of age) has led to an improved
survival rate at one year of age of greater than
80 percent compared with the 15 percent rate
observed in uncorrected patients](https://image.slidesharecdn.com/truncusarteriosus-140205113055-phpapp01/85/Truncus-arteriosus-21-320.jpg)


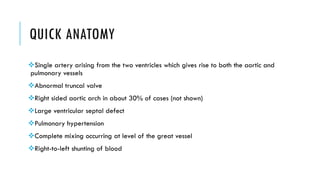
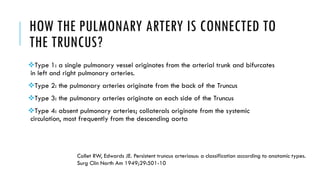
Truncus arteriosus is a rare congenital heart defect where a single arterial trunk arises from the heart to supply the pulmonary and systemic circulations. It occurs when the embryonic truncus arteriosus fails to divide into the aorta and pulmonary artery. Left untreated, it causes cyanosis and heart failure in newborns. Surgical repair is now possible to connect the pulmonary artery to the right ventricle, improving survival rates to over 80% at one year of age compared to just 15% for uncorrected patients.