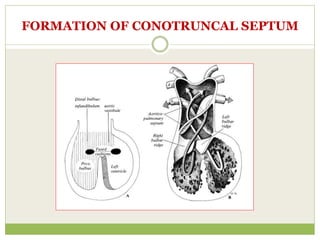
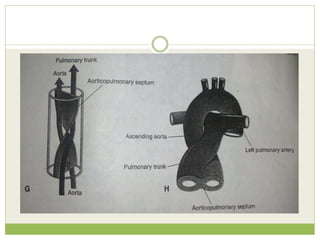
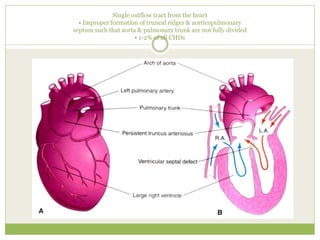
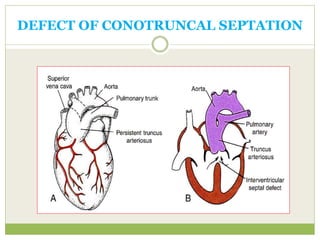
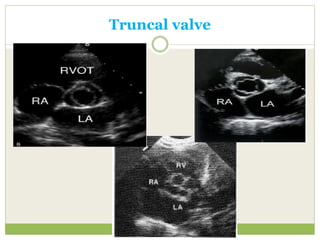
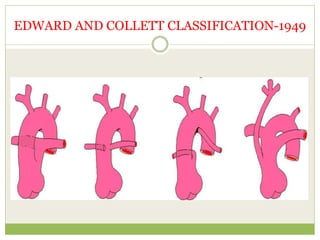
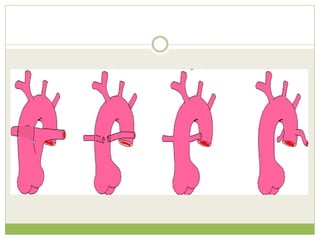
Truncus arteriosus is a rare congenital heart defect characterized by a single outflow tract from the heart due to improper formation of the truncal ridges and aorticopulmonary septum. This condition frequently occurs in conjunction with syndromes like DiGeorge's syndrome and is classified into types based on the origin of the pulmonary arteries. Echocardiography plays a critical role in diagnosis and management, revealing potential associated anomalies and allowing for evaluation of the truncal valve.