Downloaded 317 times
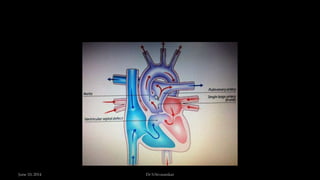
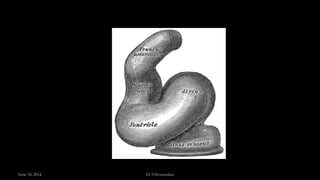
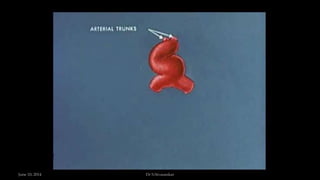
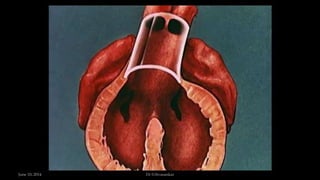
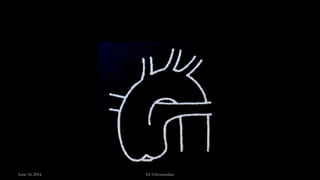
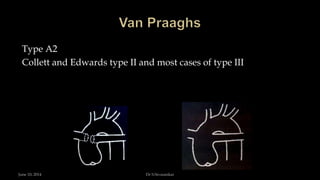
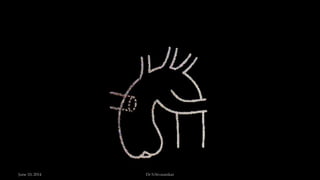
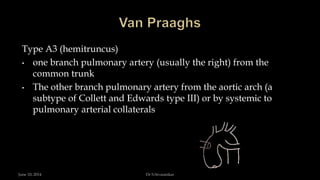
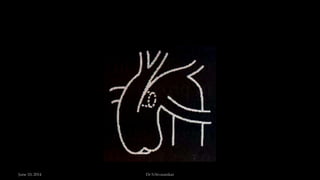

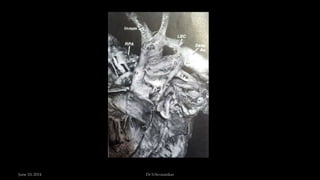
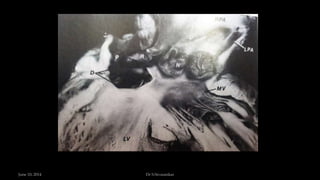


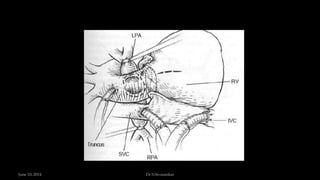
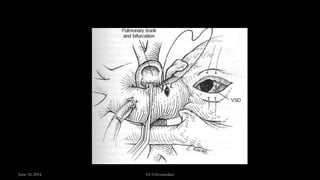


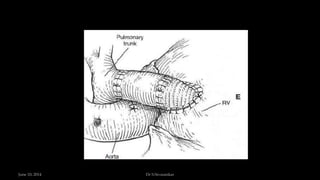
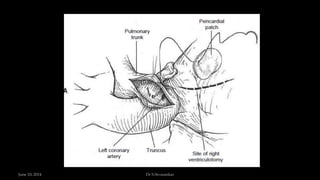
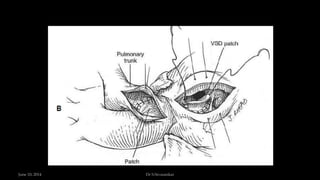
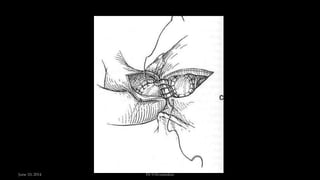
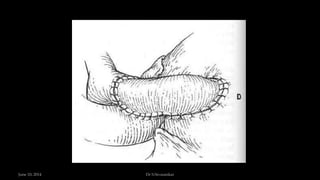
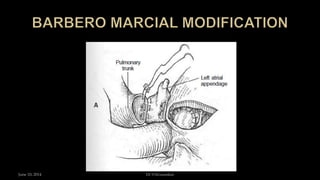
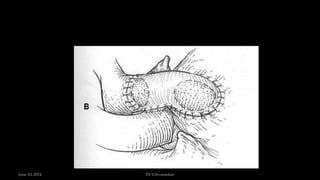
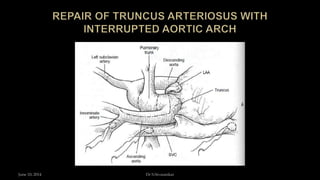
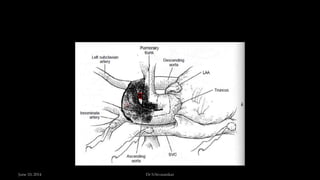

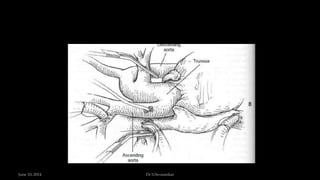
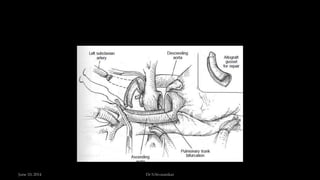
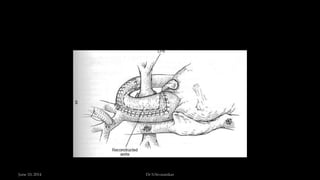
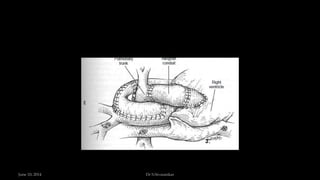


This document discusses persistent truncus arteriosus, a congenital heart defect where a single arterial trunk arises from the heart to provide blood flow to the systemic, pulmonary, and coronary circulations. It describes the embryology, anatomy, classification, presentation, diagnosis, and treatment of the condition. Surgical repair aims to close the ventricular septal defect, commit the common trunk to the left ventricle, and reconstruct the right ventricular outflow tract. Outcomes have improved with early corrective surgery, though additional anomalies increase mortality risk.