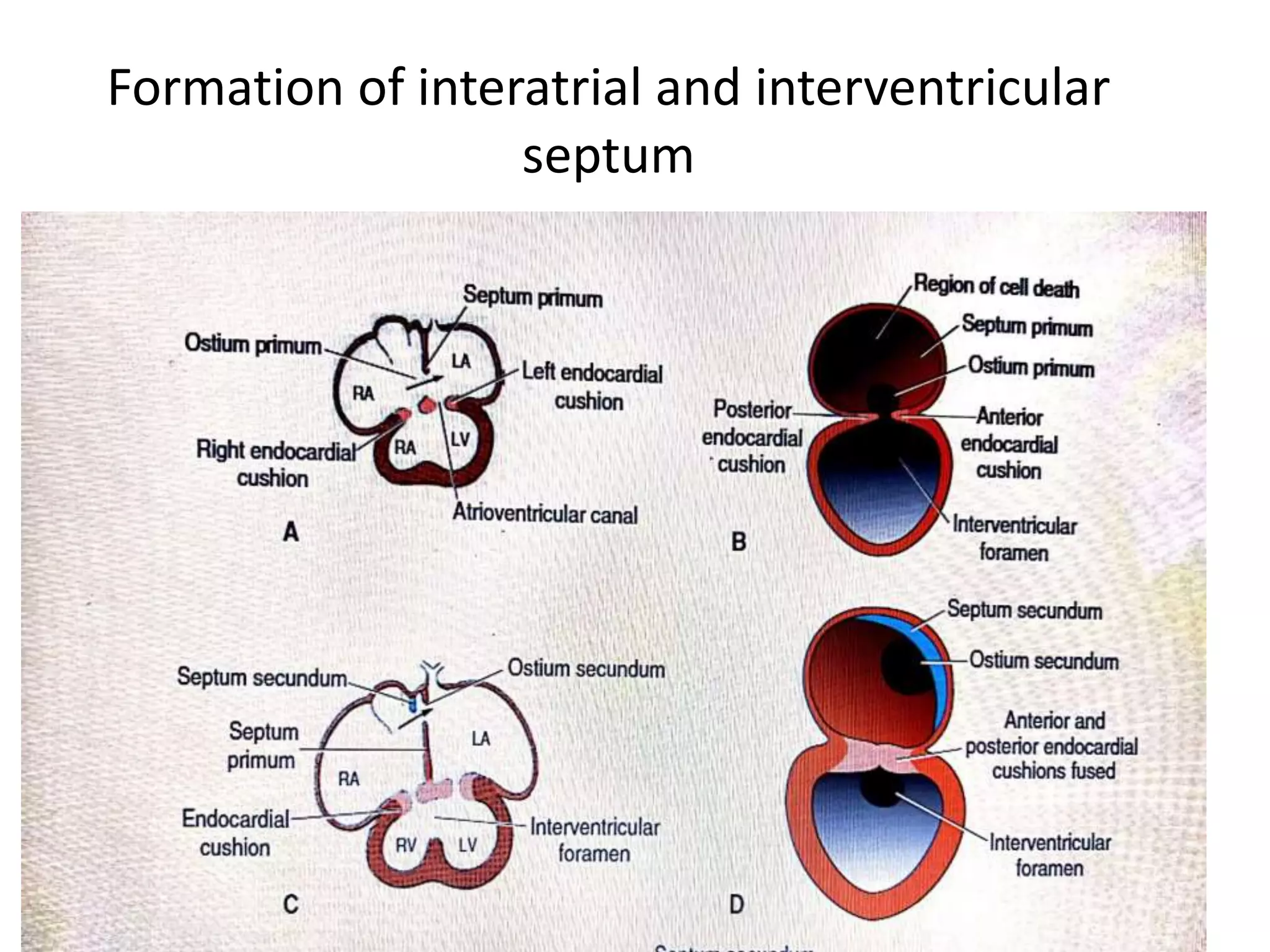
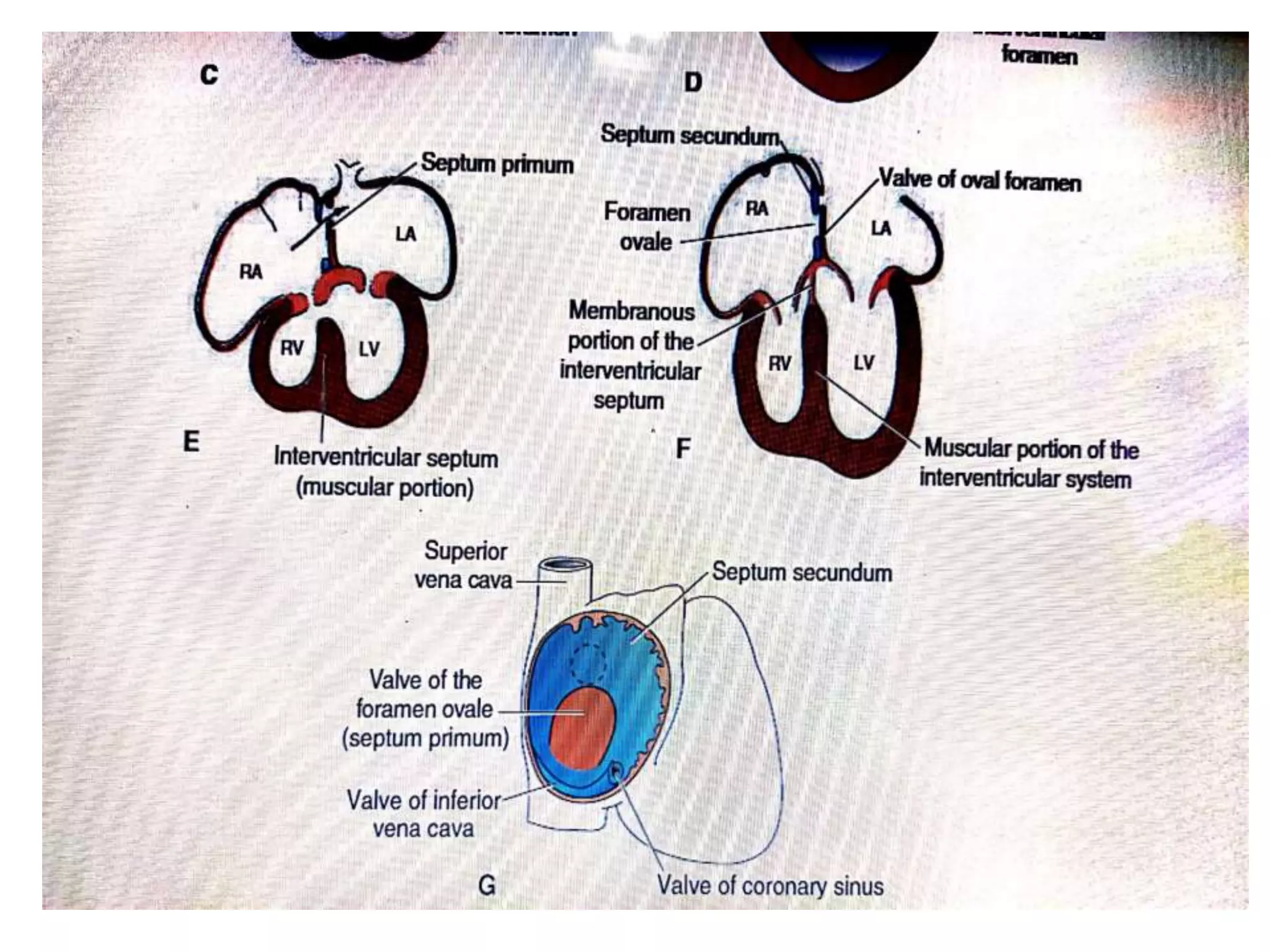
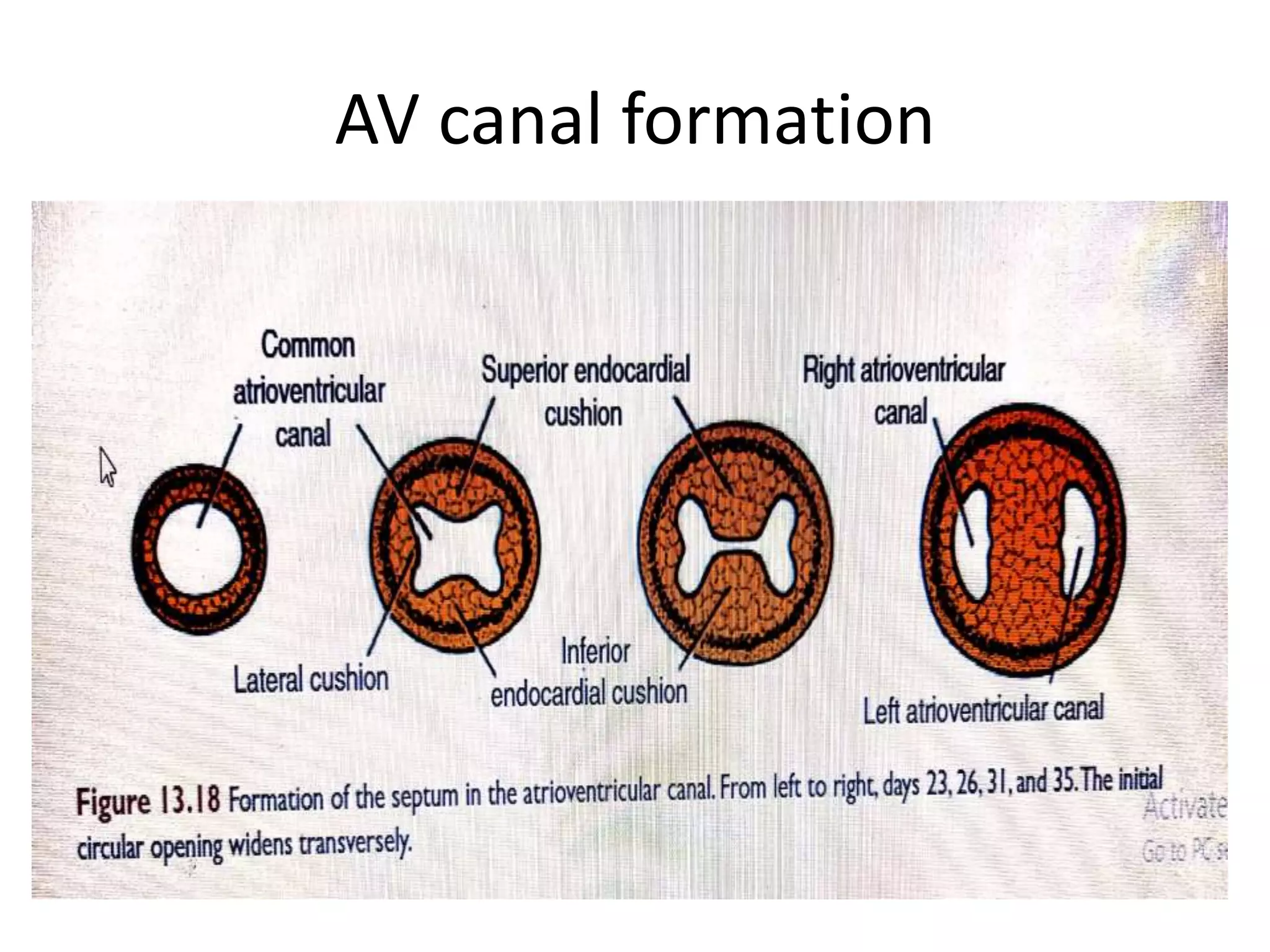
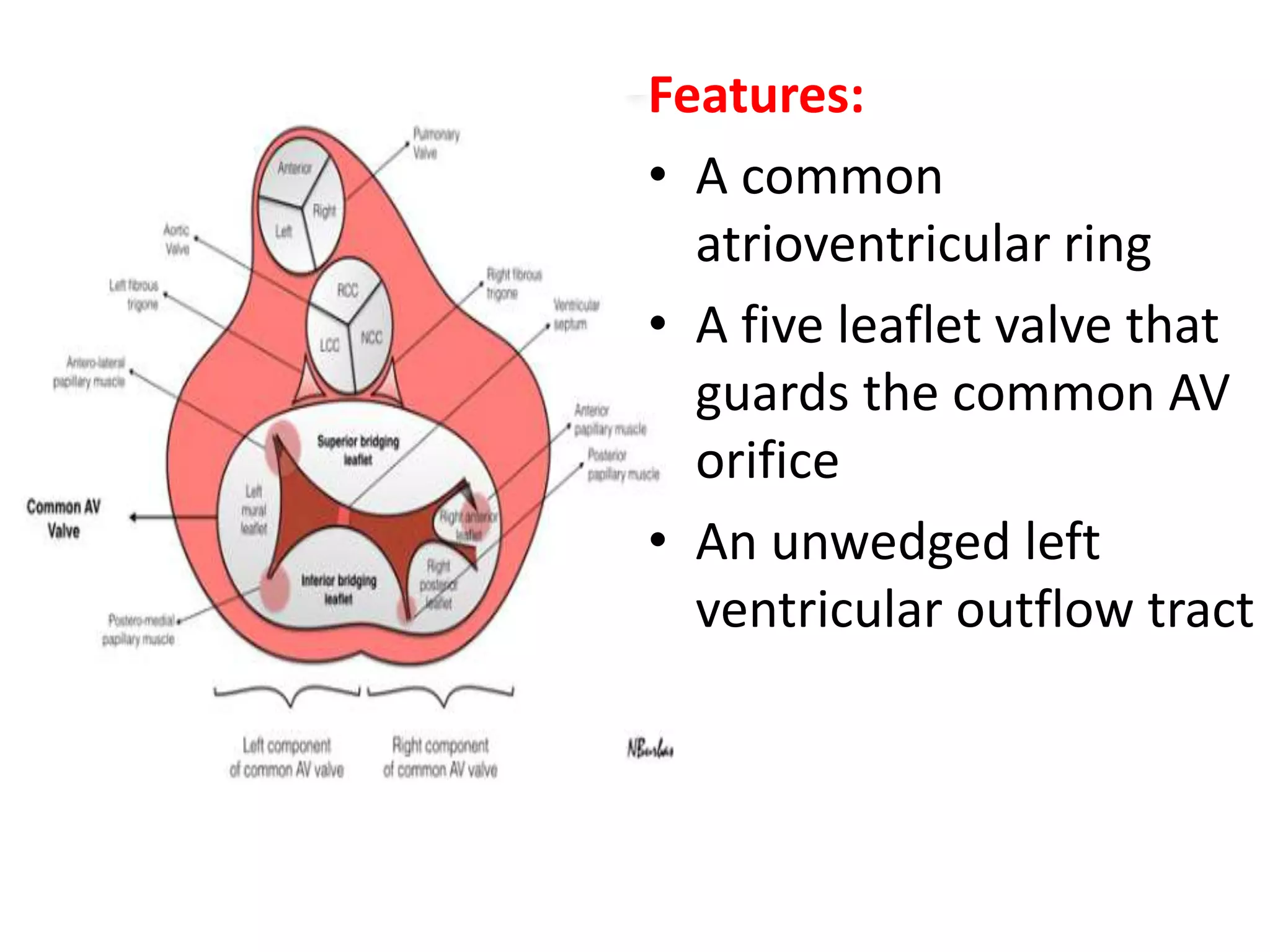
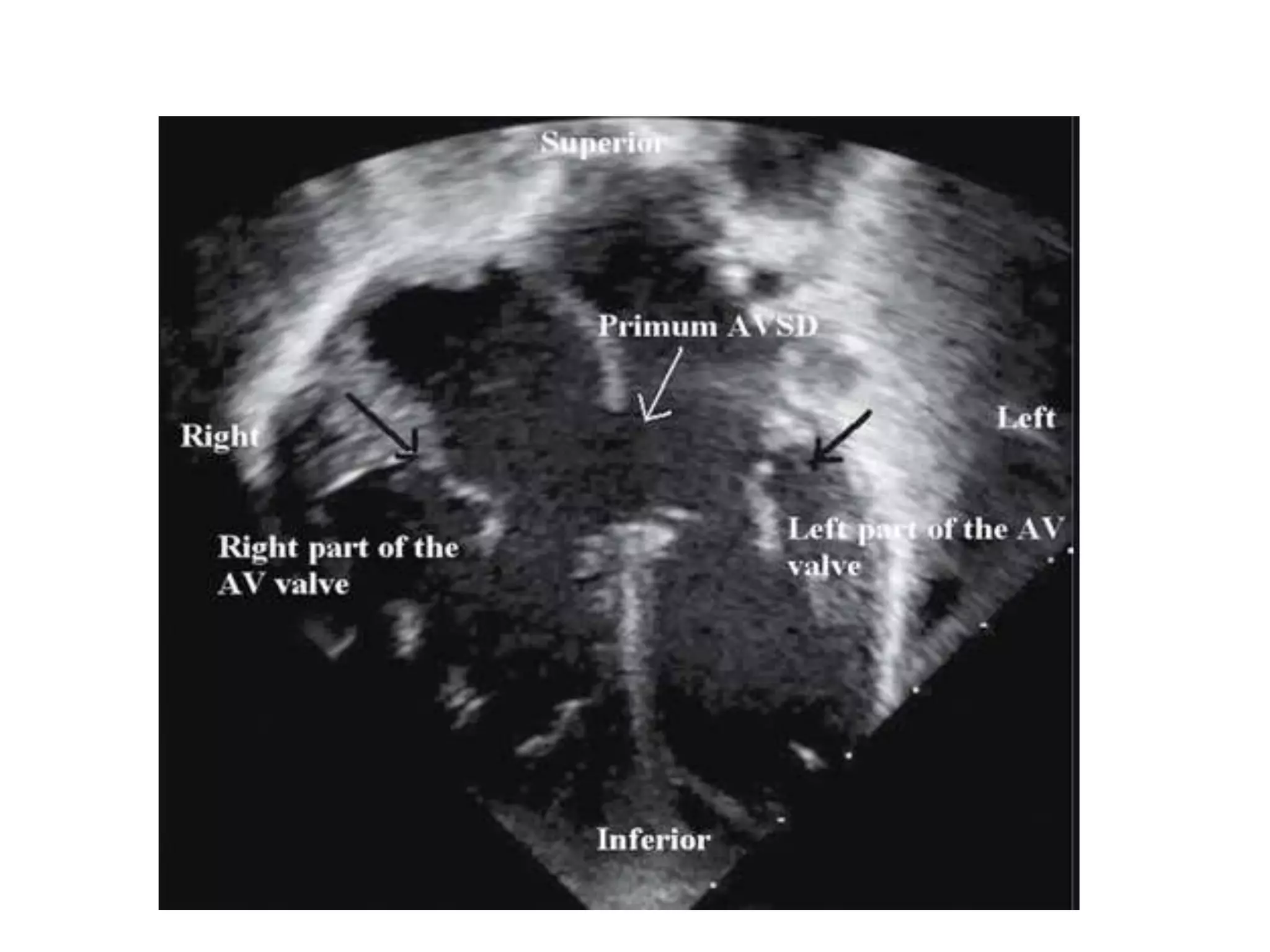
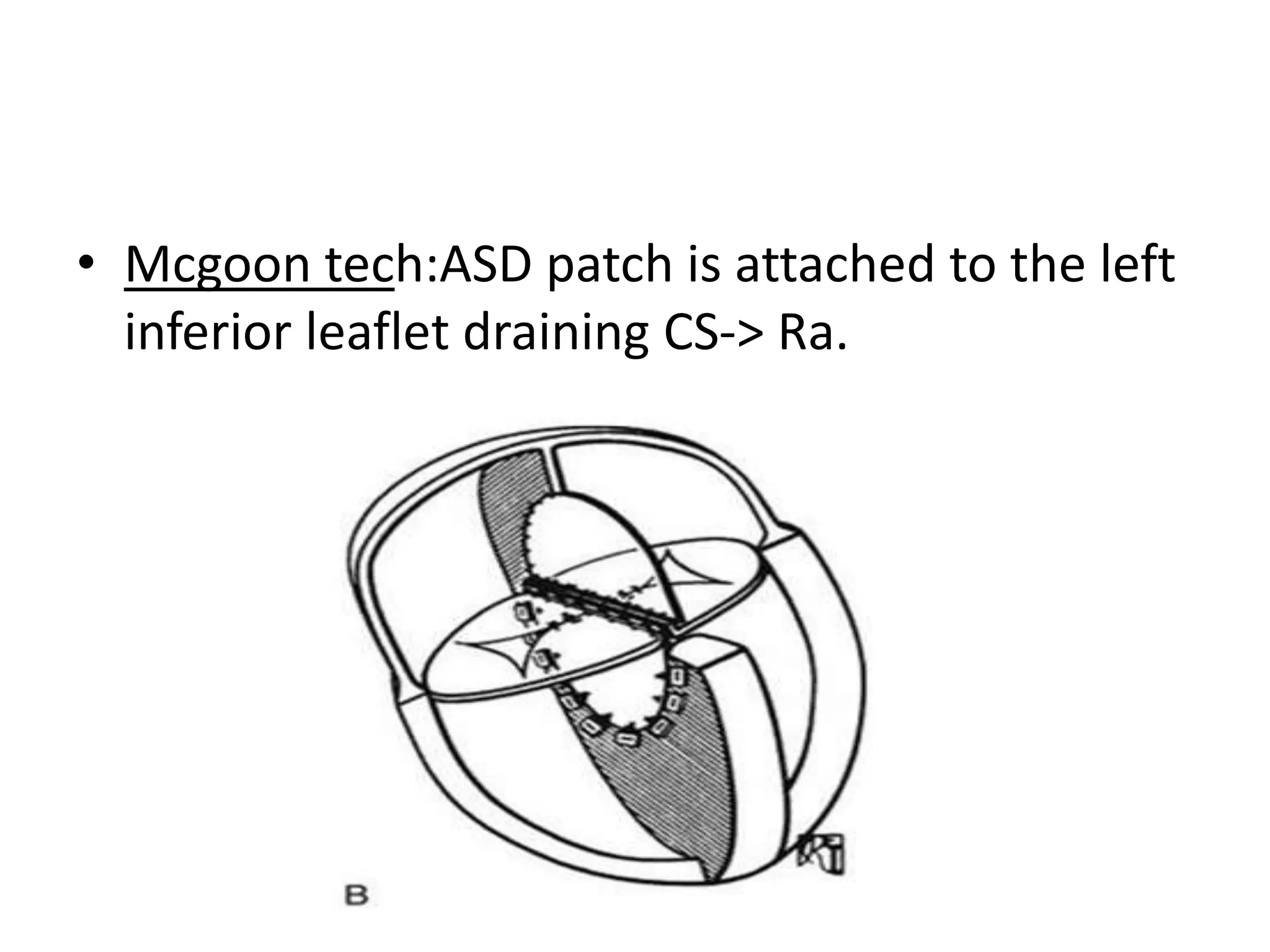
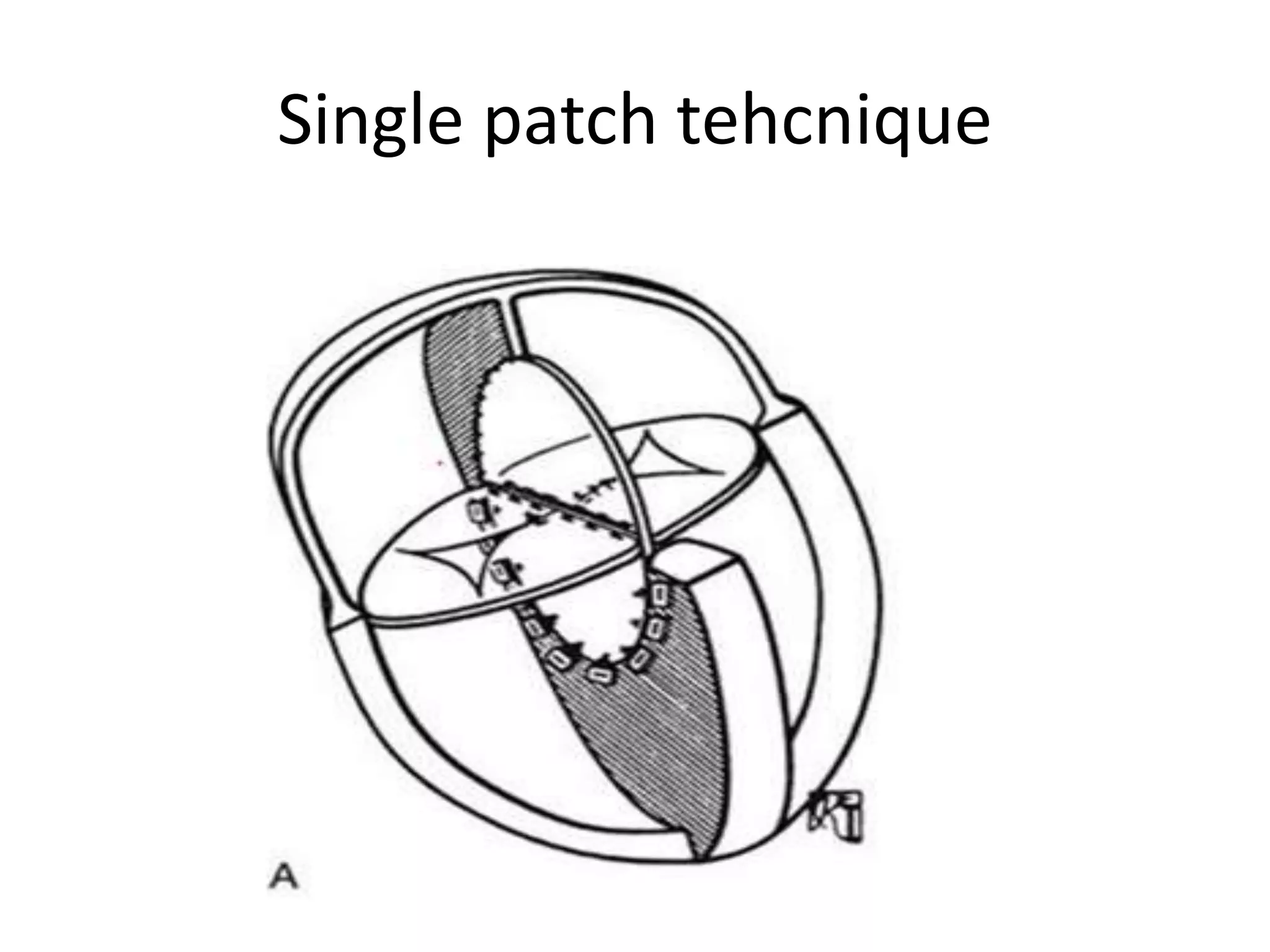
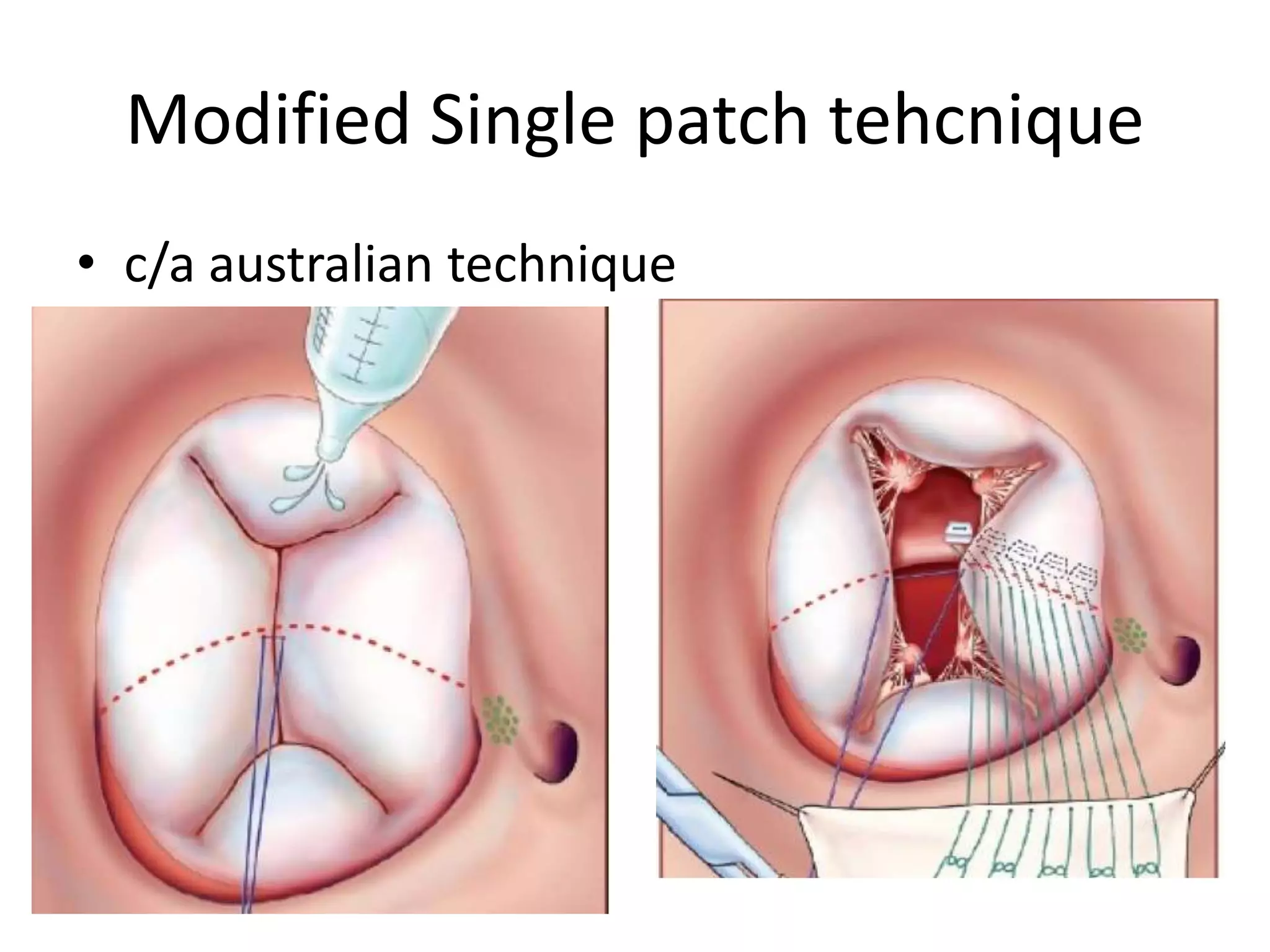
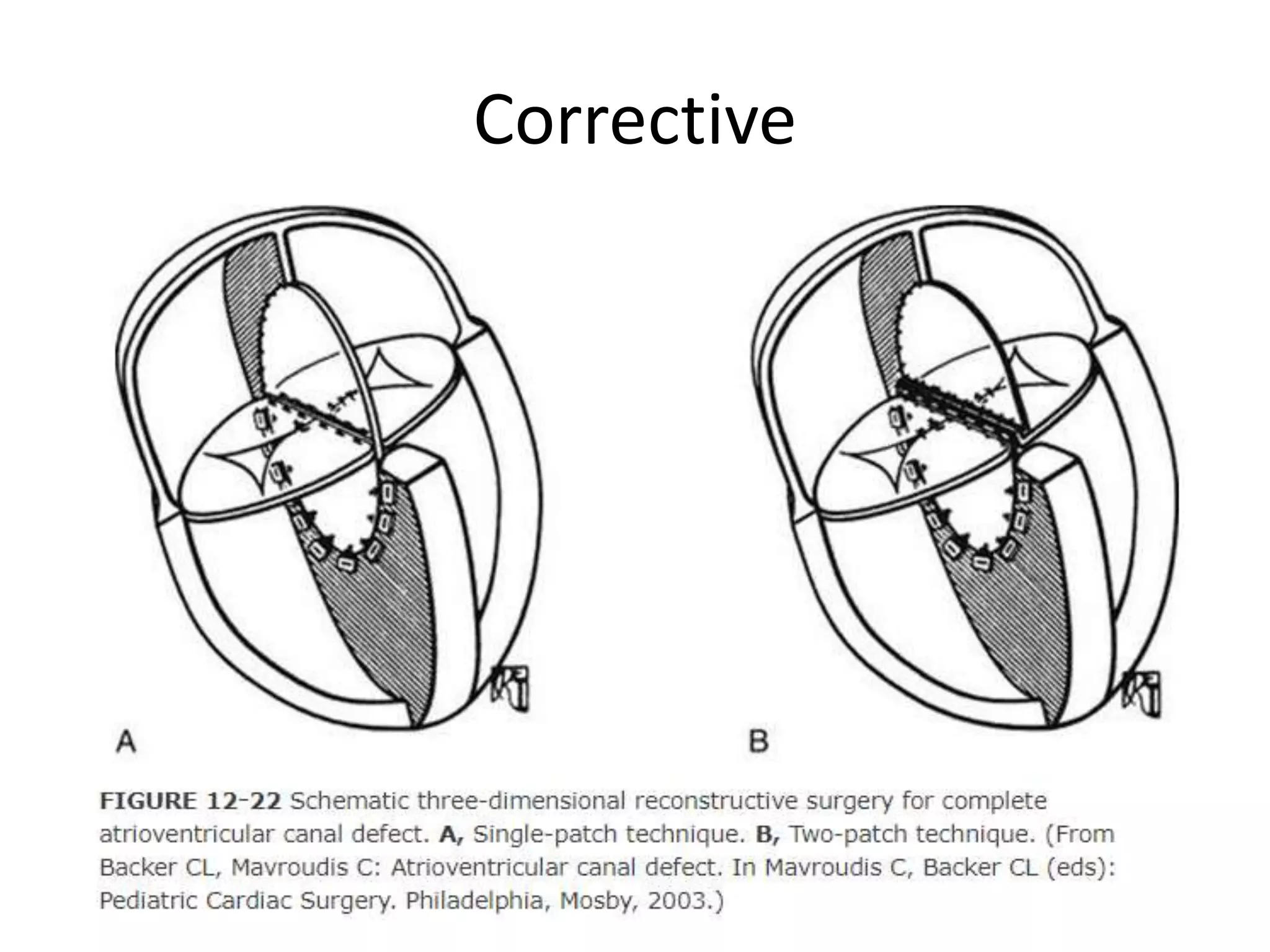
An atrioventricular canal defect, also known as an endocardial cushion defect, is characterized by a complete absence of the atrioventricular septum. It results from abnormal differentiation and remodeling of endocardial cushion mesenchyme that fails to form the septal tissue. It presents with a common atrioventricular ring, a five leaflet valve guarding the common AV orifice, and an unwedged left ventricular outflow tract. Surgical repair is usually done between 2 to 4 months of age to close the septal defects and reconstruct the valves. Techniques include single patch, double patch, and modified single patch closure.