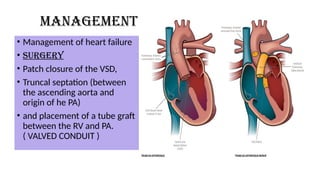
The document discusses truncus arteriosus and transposition of great vessels, two rare congenital heart diseases characterized by abnormal connections between the heart and major arteries, affecting blood flow to the body and lungs. It outlines causes, risk factors, types, clinical manifestations, diagnostic studies, and management options, emphasizing the need for surgical interventions and ongoing medical care. Prognosis varies by condition, with survival rates for surgical treatments being relatively high, although long-term complications may occur.






























































![Acute_respiratory_failure[1] [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/acuterespiratoryfailure1autosaved-240613055024-837043a9-thumbnail.jpg?width=640&height=640&fit=bounds)



























