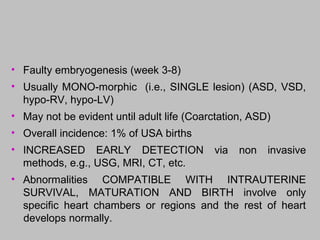
• Faulty embryogenesis(week 3-8)
• Usually MONO-morphic (i.e., SINGLE lesion) (ASD, VSD,
hypo-RV, hypo-LV)
• May not be evident until adult life (Coarctation, ASD)
• Overall incidence: 1% of USA births
• INCREASED EARLY DETECTION via non invasive
methods, e.g., USG, MRI, CT, etc.
• Abnormalities COMPATIBLE WITH INTRAUTERINE
SURVIVAL, MATURATION AND BIRTH involve only
specific heart chambers or regions and the rest of heart
develops normally.
4.
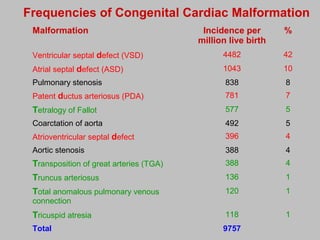
Malformation Incidence per
millionlive birth
%
Ventricular septal defect (VSD) 4482 42
Atrial septal defect (ASD) 1043 10
Pulmonary stenosis 838 8
Patent ductus arteriosus (PDA) 781 7
Tetralogy of Fallot 577 5
Coarctation of aorta 492 5
Atrioventricular septal defect 396 4
Aortic stenosis 388 4
Transposition of great arteries (TGA) 388 4
Truncus arteriosus 136 1
Total anomalous pulmonary venous
connection
120 1
Tricuspid atresia 118 1
Total 9757
Frequencies of Congenital Cardiac Malformation
5.
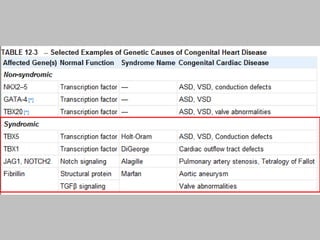
GENETICS
• Gene abnormalitiesin only 10% of CHD
• Trisomies 21 (Down’s Syndrome), 13, 15, 18,
XO
• GATA4, TBX5, and NKX2-5, three transcription factors,
are mutated in some patients with atrial and ventricular
septal defects
• Region of chromosome 22 important in heart
development … 22q11.2 deletion
CHD
• LR SHUNTS:all “D’s” in their names
– NO cyanosis
– PULMONARY HYPERTENSION
– Significant pulmonary hypertension is irreversible
• RL SHUNTS: all “T’s” in their names
– CYANOSIS (i.e. “blue” babies)
– VENOUS EMBOLI become SYSTEMIC (i.e.
paradoxical)
• OBSTRUCTIONS
9.
CYANOSIS IN CHILDREN
•Central cyanosis:
Cyanosis of the tongue, mucous membranes and
peripheral skin, it is necessary to have >3g/dl of reduced
Hb to have it.
• Peripheral cyanosis:
It is visible only in the skin of the extremities with normal
arterial saturation due to vasomotor instability, ex. cold
environment.
10.
• Left-to-Right shuntsinduce
– chronic right-sided volume overload
– secondary pulmonary hypertension
– right ventricle hypertrophy
– right-sided pressures exceed left-sided
pressures and the shunt becomes right to
left.
– cyanosis appears late (late cyanotic
congenital heart disease, or Eisenmenger
syndrome). .
LR
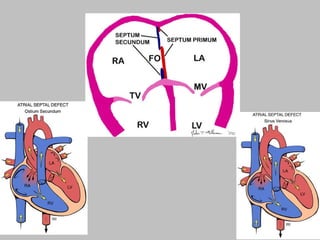
ASD
• Usually asymptomaticuntil adulthood (>30y)
• SECUNDUM (90%): Defective fossa ovalis; single,
multiple or fenestrated.
• PRIMUM (5%): Next to AV valves, mitral cleft; common
in Down syndrome
• SINUS VENOSUS (5%): Next to SVC with anomalous
pulmonary veins draining to SVC or RA
VSD
• By far,most common CHD defect
• Only 30% are isolated.
• Often with TETRALOGY of FALLOT
• 90% involve the membranous septum.
• If muscular septum is involved, likely to have multiple
holes.
• SMALL ones often close spontaneously
• LARGE ones progress to pulmonary hypertension.
• Greater risk for infective endocarditis.
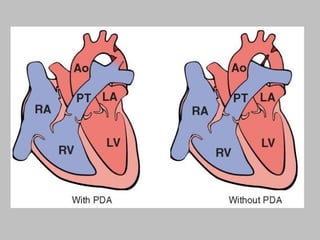
PDA
• At birthunder the influence of higher oxygen tensions
and reduced local prostaglandin E synthesis, muscular
contraction normally closes the ductus within 1 or 2 days
of life. (Persistent patency beyond that point is generally
permanent)
• 90% isolated
• HARSH, machinery-like murmur
• Closing the defect may be life saving
• Keeping it open may be life saving
– Why?
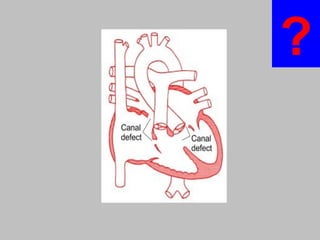
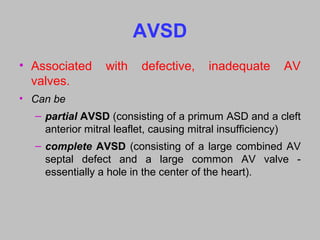
AVSD
• Associated withdefective, inadequate AV
valves.
• Can be
– partial AVSD (consisting of a primum ASD and a cleft
anterior mitral leaflet, causing mitral insufficiency)
– complete AVSD (consisting of a large combined AV
septal defect and a large common AV valve -
essentially a hole in the center of the heart).
22.
RL
(Cyanotic Congenital HeartDisease)
• Tetralogy of Fallot
• Transposition of great arteries
• Truncus arteriosus
• Total anomalous pulmonary venous connection
• Tricuspid atresia
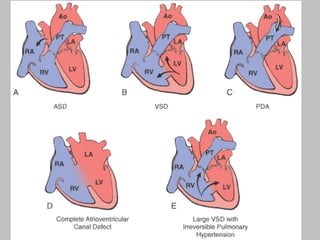
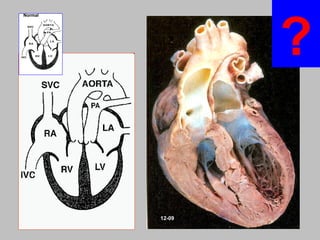
Normal
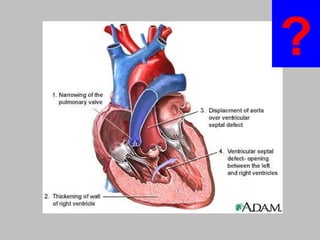
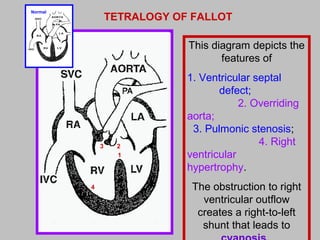
This diagram depictsthe
features of
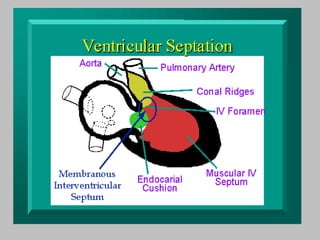
1. Ventricular septal
defect;
2. Overriding
aorta;
3. Pulmonic stenosis;
4. Right
ventricular
hypertrophy.
The obstruction to right
ventricular outflow
creates a right-to-left
shunt that leads to
TETRALOGY OF FALLOT
1
23
4
25.
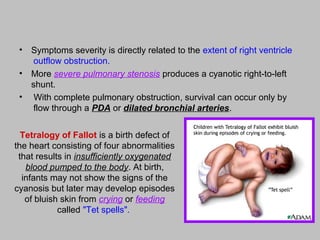
Tetralogy of Fallotis a birth defect of
the heart consisting of four abnormalities
that results in insufficiently oxygenated
blood pumped to the body. At birth,
infants may not show the signs of the
cyanosis but later may develop episodes
of bluish skin from crying or feeding
called "Tet spells".
• Symptoms severity is directly related to the extent of right ventricle
outflow obstruction.
• More severe pulmonary stenosis produces a cyanotic right-to-left
shunt.
• With complete pulmonary obstruction, survival can occur only by
flow through a PDA or dilated bronchial arteries.
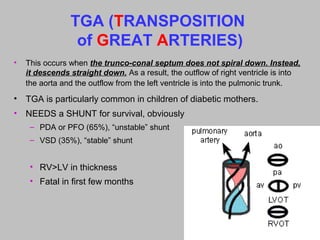
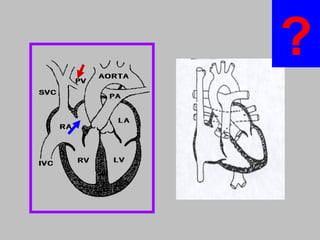
TGA (TRANSPOSITION
of GREATARTERIES)
• This occurs when the trunco-conal septum does not spiral down. Instead,
it descends straight down. As a result, the outflow of right ventricle is into
the aorta and the outflow from the left ventricle is into the pulmonic trunk.
• TGA is particularly common in children of diabetic mothers.
• NEEDS a SHUNT for survival, obviously
– PDA or PFO (65%), “unstable” shunt
– VSD (35%), “stable” shunt
• RV>LV in thickness
• Fatal in first few months
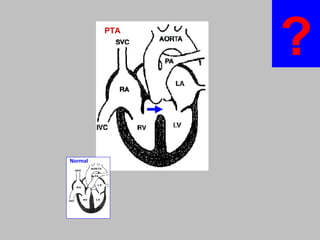
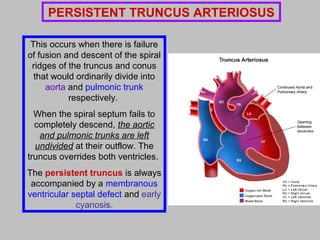
This occurs whenthere is failure
of fusion and descent of the spiral
ridges of the truncus and conus
that would ordinarily divide into
aorta and pulmonic trunk
respectively.
When the spiral septum fails to
completely descend, the aortic
and pulmonic trunks are left
undivided at their outflow. The
truncus overrides both ventricles.
The persistent truncus is always
accompanied by a membranous
ventricular septal defect and early
cyanosis.
PERSISTENT TRUNCUS ARTERIOSUS
Total Anomalous PulmonaryVenous
Connection (TAPVC)
• PULMONARY VEINS do NOT go into LA, but into L.
innominate vein or coronary sinus
• Needs a PFO or a VSD
• Hypoplastic LA
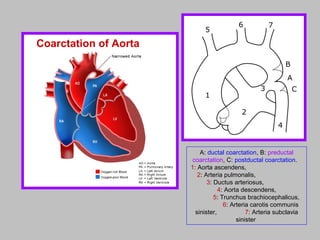
COARCTATION of AORTA
•M>F … but XO’s frequently have it
• INFANTILE FORM (proximal to PDA) … most common …
SERIOUS
• ADULT FORM (CLOSED DUCTUS, i.e., No PDA)
• Bicuspid aortic valve … 50% of the time
• There is upper extremity hypertension but lower extremity
hypotension with arterial insufficiency (claudication, cold
sensitivity)
• Collateral flow around the coarctation generally develops via
internal mammary and axillary artery dilation with intercostal
rib notching notable on X-rays.
38.
Rt PA
Lt PA
PA
A:ductal coarctation, B: preductal
coarctation, C: postductal coarctation.
1: Aorta ascendens,
2: Arteria pulmonalis,
3: Ductus arteriosus,
4: Aorta descendens,
5: Trunchus brachiocephalicus,
6: Arteria carotis communis
sinister, 7: Arteria subclavia
sinister
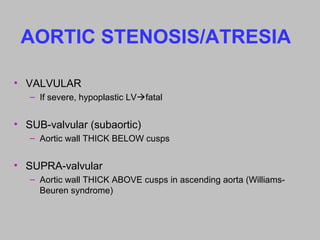
Coarctation of Aorta
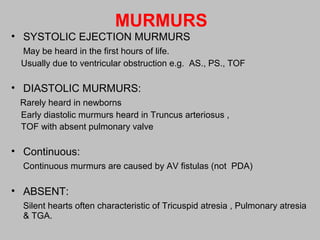
MURMURS
• SYSTOLIC EJECTIONMURMURS
May be heard in the first hours of life.
Usually due to ventricular obstruction e.g. AS., PS., TOF
• DIASTOLIC MURMURS:
Rarely heard in newborns
Early diastolic murmurs heard in Truncus arteriosus ,
TOF with absent pulmonary valve
• Continuous:
Continuous murmurs are caused by AV fistulas (not PDA)
• ABSENT:
Silent hearts often characteristic of Tricuspid atresia , Pulmonary atresia
& TGA.
45.
USEFUL HINTS
• Largebaby with rapid, shallow abdominal breathing: D-TGA
• Upper body blue, lower body pink; seen in : D-GA + PDA.
• Only cyanotic newborn who has a thrill: Tricuspid atresia.
• Ejection click is often heard in : Severe PS, HLHS
• Systolic ejection murmurs in first hours of life: TOF, PS, AS
• Silent heart characteristic of : D-TGA, Pulmonary atresia.
• Pulse oximetry& ABG should be obtained from the RIGHT
arm.
• ECG showing LEFT axis deviation: Tricuspid atresia
46.
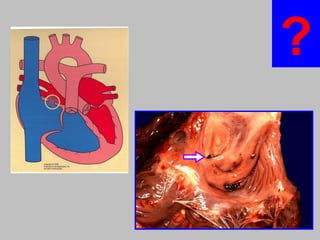
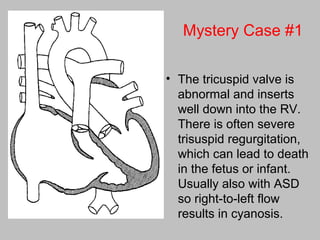
Mystery Case #1
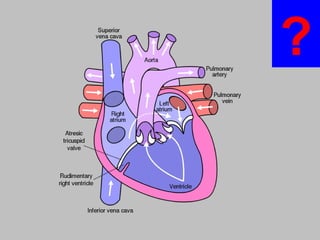
•The tricuspid valve is
abnormal and inserts
well down into the RV.
There is often severe
trisuspid regurgitation,
which can lead to death
in the fetus or infant.
Usually also with ASD
so right-to-left flow
results in cyanosis.
47.
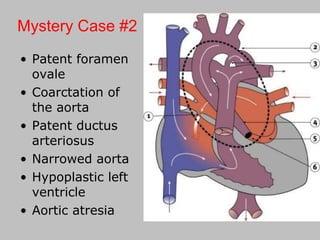
• Patent foramen
ovale
•Coarctation of
the aorta
• Patent ductus
arteriosus
• Narrowed aorta
• Hypoplastic left
ventricle
• Aortic atresia
Mystery Case #2
Editor's Notes
#3 hypo-plasia if it occurs before birth and atrophy if it develops postnatally.
#5 Twelve disorders account for about 85% of cases
#7 deletion of chromosome 22q11.2, which is found in up to 50% of patients with DiGeorge syndrome. In this syndrome the fourth branchial arch and the derivatives of the third and fourth pharyngeal pouches, which contribute to the formation of the thymus, parathyroids, and heart, develop abnormally. One candidate gene in the deleted region is TBX1, which encodes a transcription factor that regulates the expansion of cardiac progenitors in the second heart field.
#9 Moreover, with right-to-left shunts, emboli arising in peripheral veins can bypass the lungs and directly enter the systemic circulation (paradoxical embolism);
#11 Prolonged pulmonary arterial vasoconstriction, however, stimulates the proliferation of the vascular wall cells and the consequent development of irreversible obstructive intimal lesions analogous to the arteriolar changes seen in systemic hypertension ( Chapter 11 ). Eventually, pulmonary vascular resistance approaches systemic levels, thereby producing a new right-to-left shunt that introduces unoxygenated blood into the systemic circulation (late cyanotic congenital heart disease, or Eisenmenger syndrome).
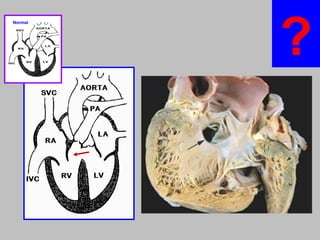
#13 In the region of the foramen ovale on the interatrial septum is a small atrial septal defect, as seen in this heart opened on the right side (Rt atrium). Here the defect is not closed by the septum secundum, so a shunt exists across from left to right.
#23 All the RL congenital shunts are CYANOTIC, and have T’s in their names.
CYANOSIS means UN-oxygenated blood is BYPASSING the lungs.
#27 Right ventricular hypertrophy becomes prominent because this chamber functions as the systemic ventricle. Concurrently the left ventricle becomes thin-walled as it sports the low resistance pulmonary circulation. Thinning of left ventricle.
#29 In TRUNCUS ARTERIOSUS, the embryological structure known as the truncus arteriosus fails to properly divide into the pulmonary trunk and aorta
#33 the pulmonary veins do not return to the left atrium, but connect to the innominate vein, coronary sinus, or some other anomalous site. There is overload of the right heart. In the case shown here, an atrial septal defect provides for flow of oxygenated blood to the left heart. RIGHT: opening into coronary sinus
#35 This is our THIRD category of congenital heart diseases after L—R and RL shunts.
In this THIRD type, there is NO LR or RL shunting.
#38 (1) an “infantile” form with tubular hypoplasia of the aortic arch proximal to a patent ductus arteriosus that is often symptomatic in early childhood, and (2) an “adult” form in which there is a discrete ridgelike infolding of the aorta, just opposite the closed ductus arteriosus (ligamentum arteriosum) distal to the arch vessels
#41 Can ATRESIA be thought of, anatomically, as being SEVERE stenosis? Ans: YES
#42 Complete aortic atresia is incompatible with life, but aortic stenosis may range from mild to severe
#43 deletions on chromosome 7 that include the gene for elastin. Other features of the syndrome include hypercalcemia, cognitive abnormalities, and hallmark facial anomalies (Williams-Beuren syndrome)