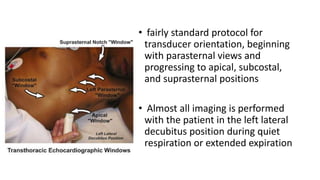
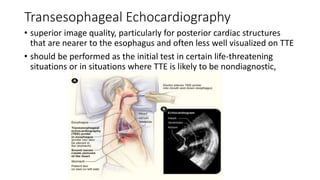
This document provides an overview of transthoracic echocardiography (TTE), including the standard views and protocols. TTE uses two-dimensional imaging to visualize the heart from various transducer positions on the chest. Standard views include parasternal, apical, subcostal, and suprasternal. Doppler echocardiography measures blood flow velocities. Continuous wave Doppler is used for high velocities while pulsed Doppler samples localized flows. Color flow Doppler maps flow direction. Three-dimensional echocardiography provides improved volume and structural assessments. Transesophageal echocardiography images the posterior heart with better quality but requires esophageal intubation.





































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)









![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

