Downloaded 376 times





![Technique
• Patients are pretreated with aspirin and possibly a calcium channel blocker to
counteract PTRA-induced vasospasm.
• glycoprotein (GP) IIb/IIIA receptor antagonists have shown benefit in limiting
speed dependent platelet activation.
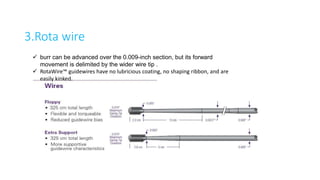
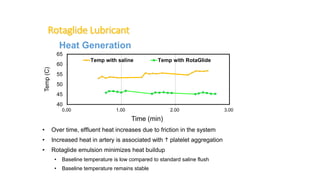
• Rotaglide™ , a lipid emulsion, can be added to the flush solution to reduce
friction, limit heat generation, and facilitate device deliverability.
Influence of a platelet GPiib/iiia receptor antagonist on myocardial hypoperfusion during rotational atherectomy as assessed by myocardial Tc-
99m sestamibi scintigraphy. ] Am Call Cardio/ 1 9 9 9 ; 3 3 : 998-1004.](https://image.slidesharecdn.com/rotablation-170407144002/85/Rotablation-11-320.jpg)


























Rotational atherectomy (RA) is a technique used for treating heavily calcified coronary lesions, developed by David Auth in the 1980s, that relies on differential cutting to prepare lesions prior to stent deployment. The procedure utilizes specialized devices like the Rotalink burr catheter and requires careful management to minimize complications such as bradycardia, dissection, and slow flow. While RA can be effective for specific cases, it carries risks and has seen a decline in usage due to the complexity and associated costs.























































































