1) Cardiac catheterization allows measurement of pressures within the heart by inserting catheters connected to transducers.
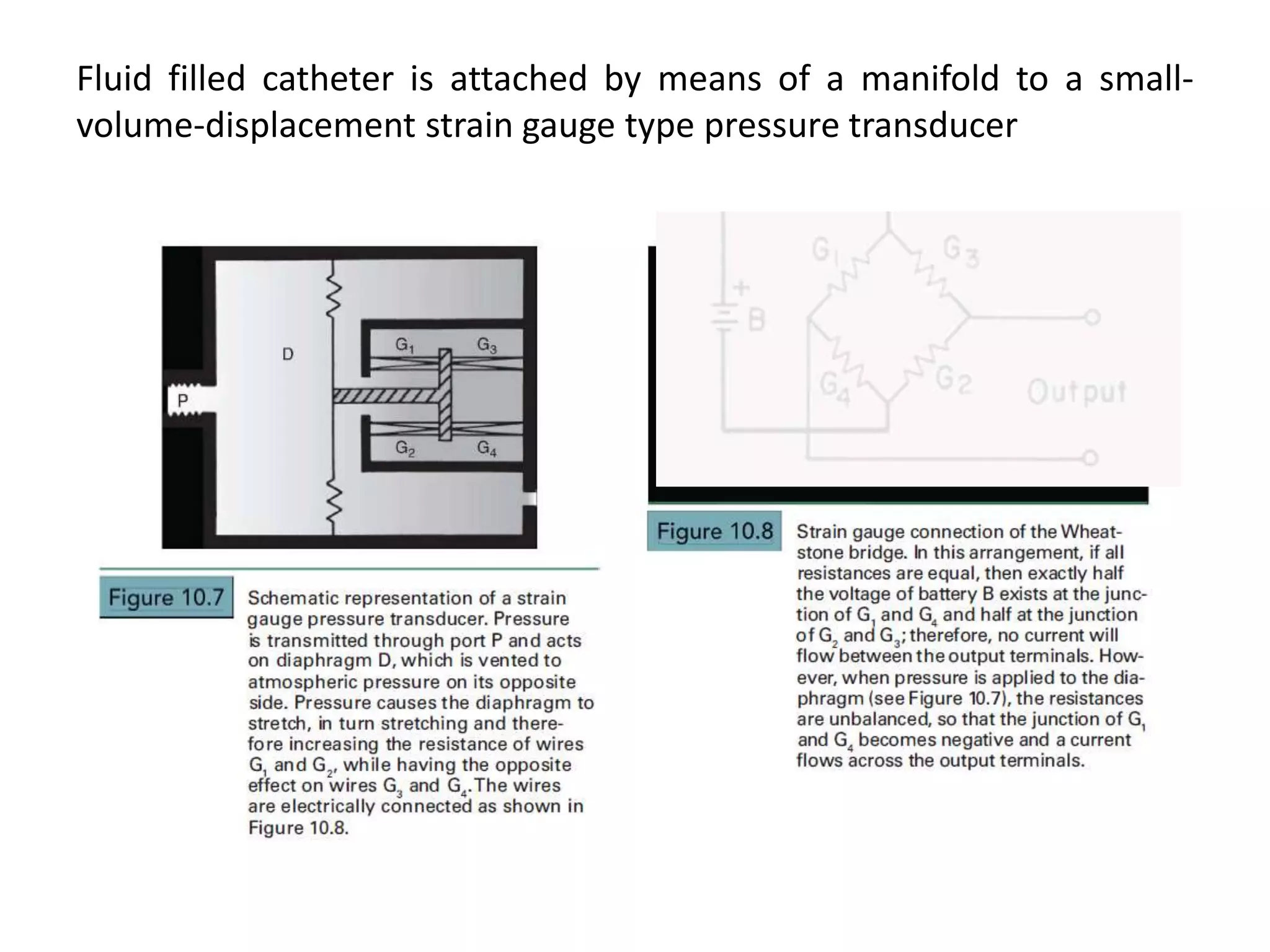
2) Proper equipment selection and setup is important to minimize artifacts and obtain accurate pressure tracings.
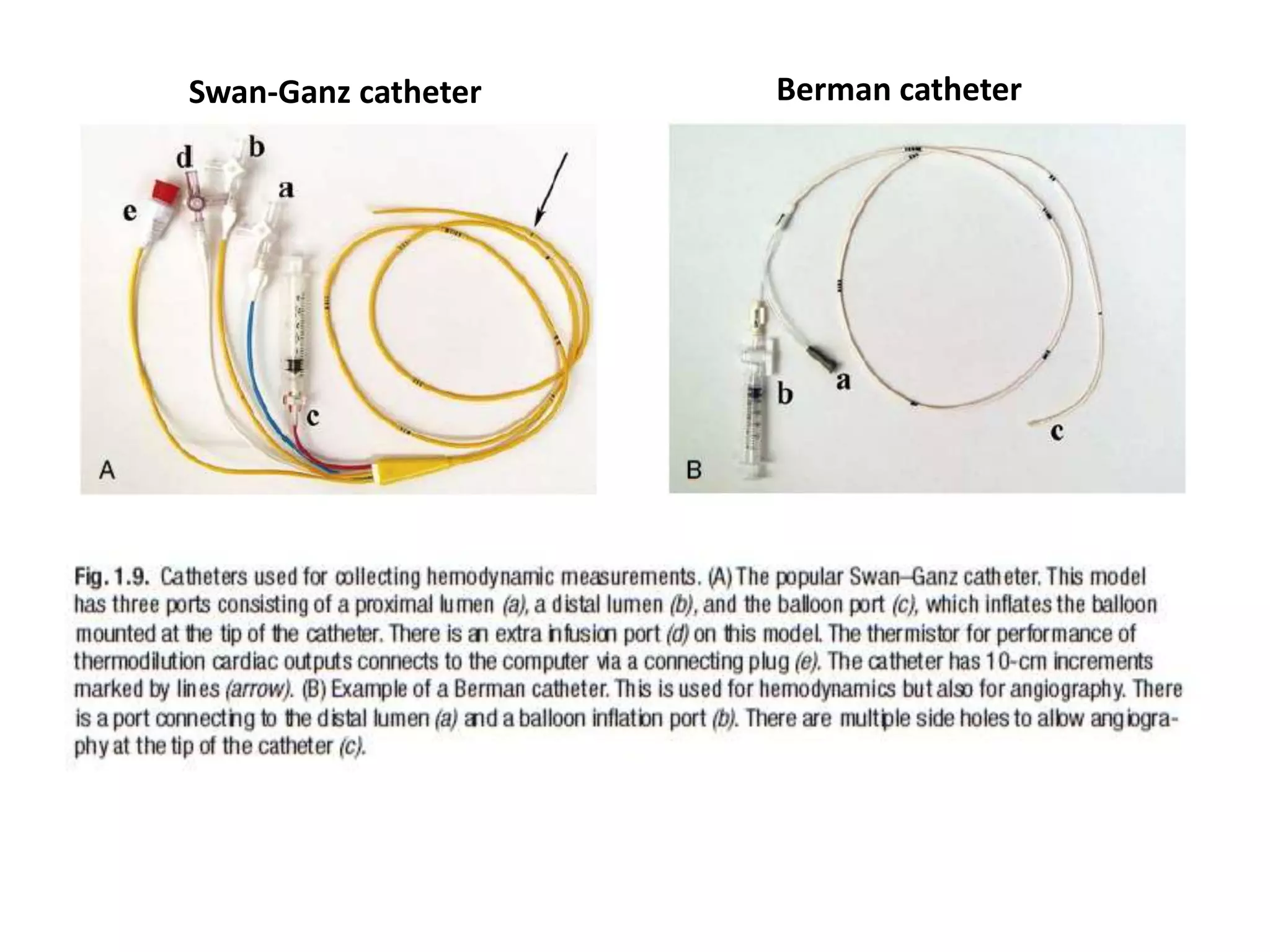
3) Different catheter types are used depending on the specific chamber being measured.