Downloaded 744 times
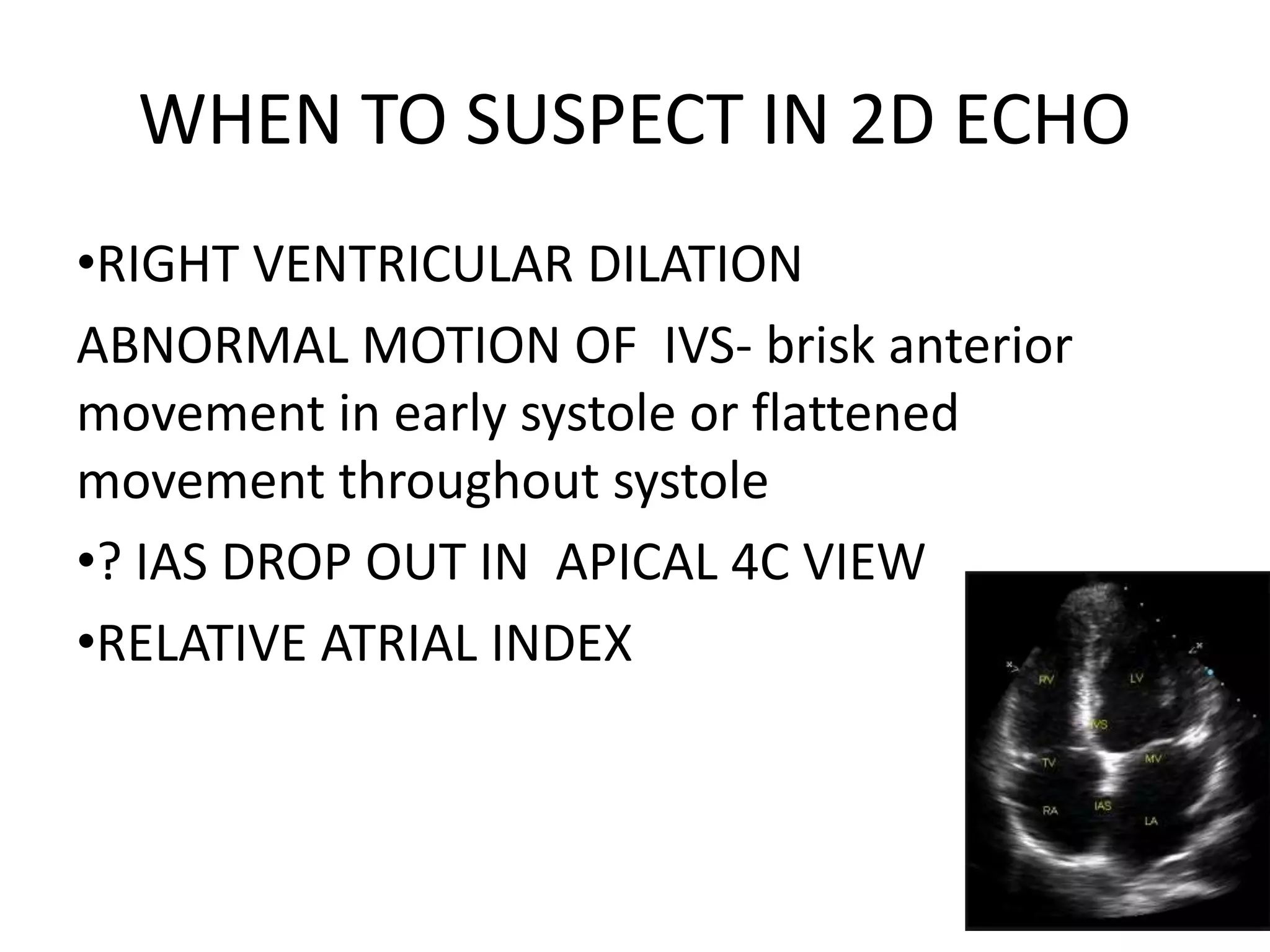
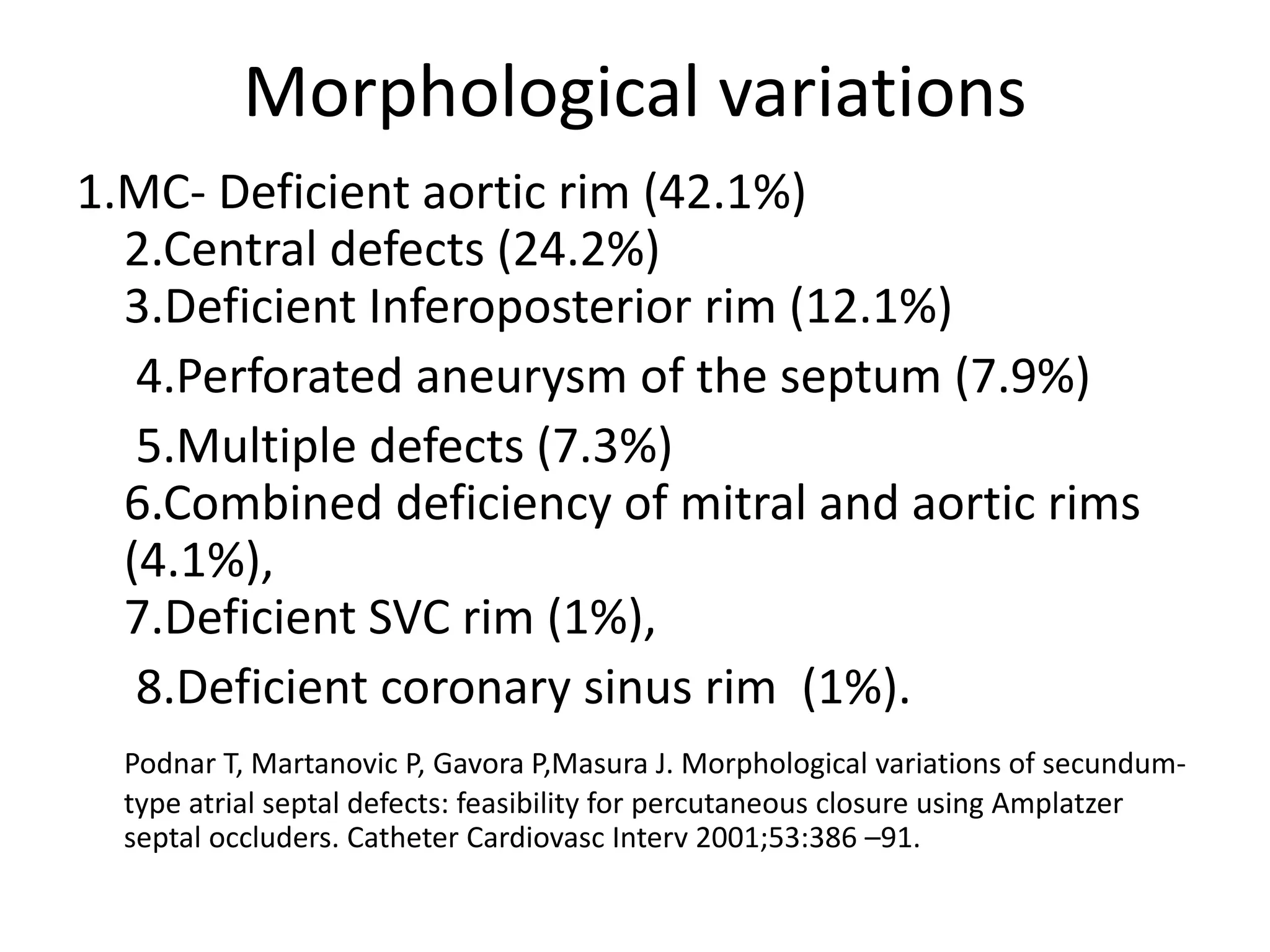
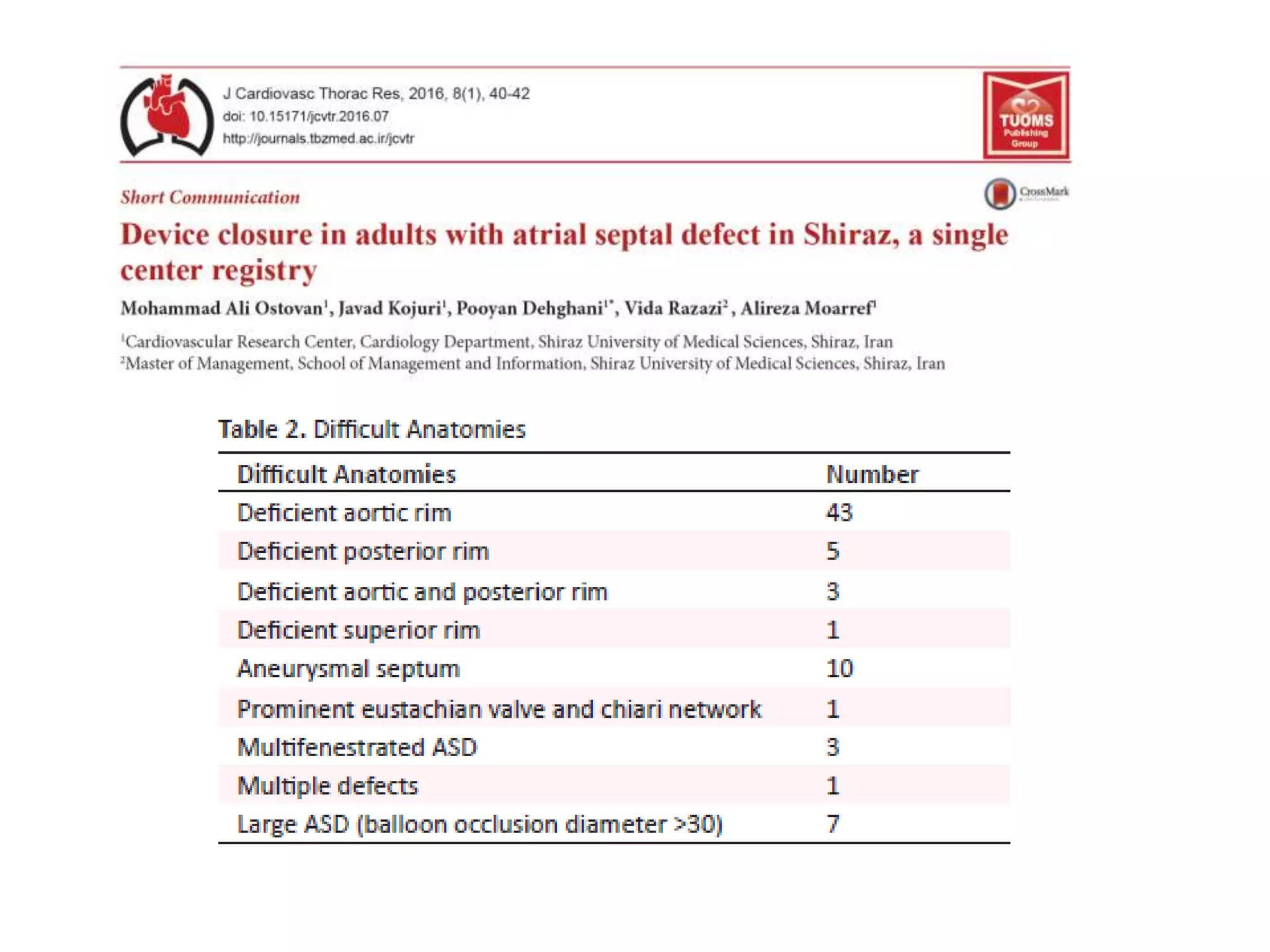
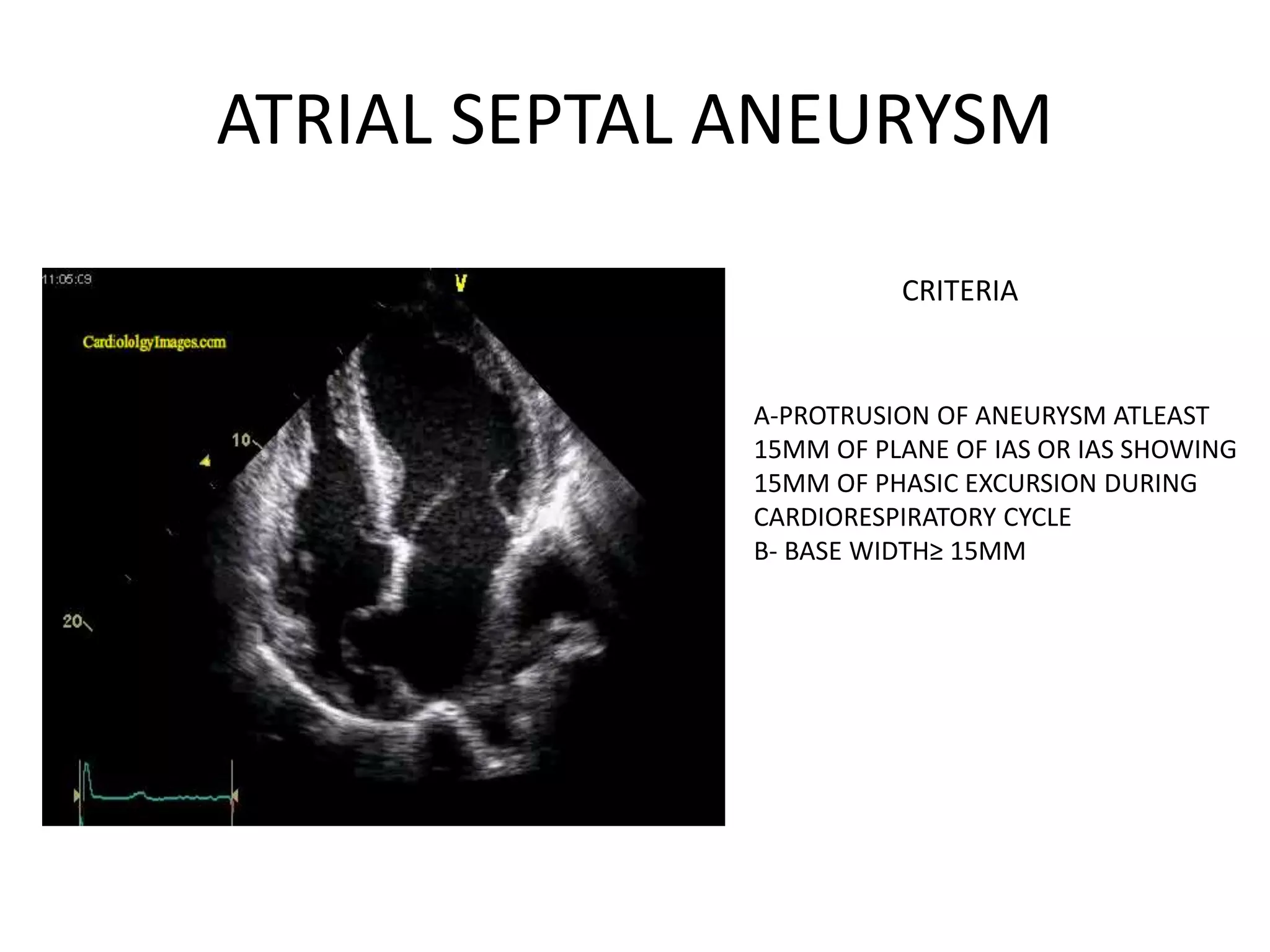
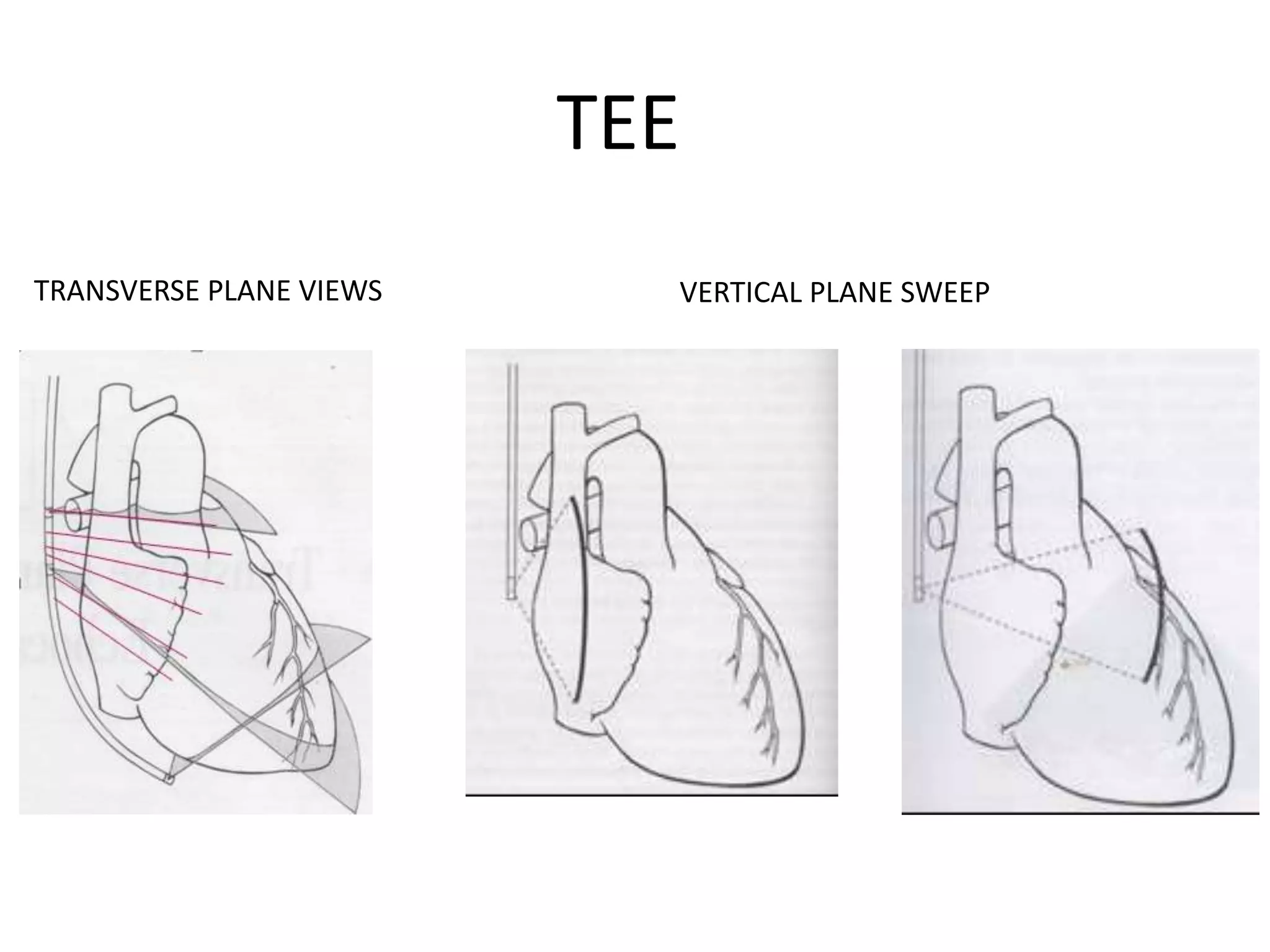
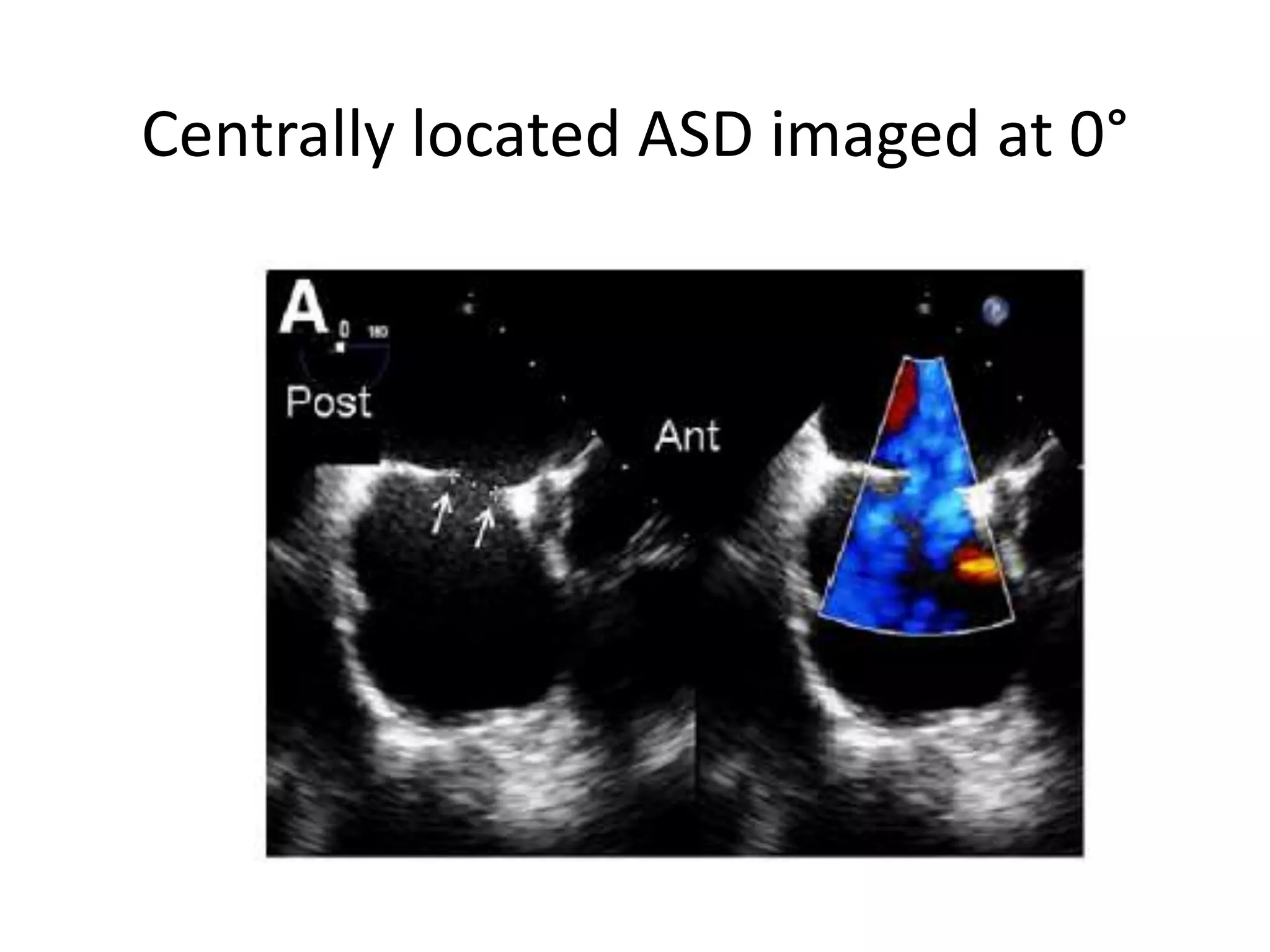


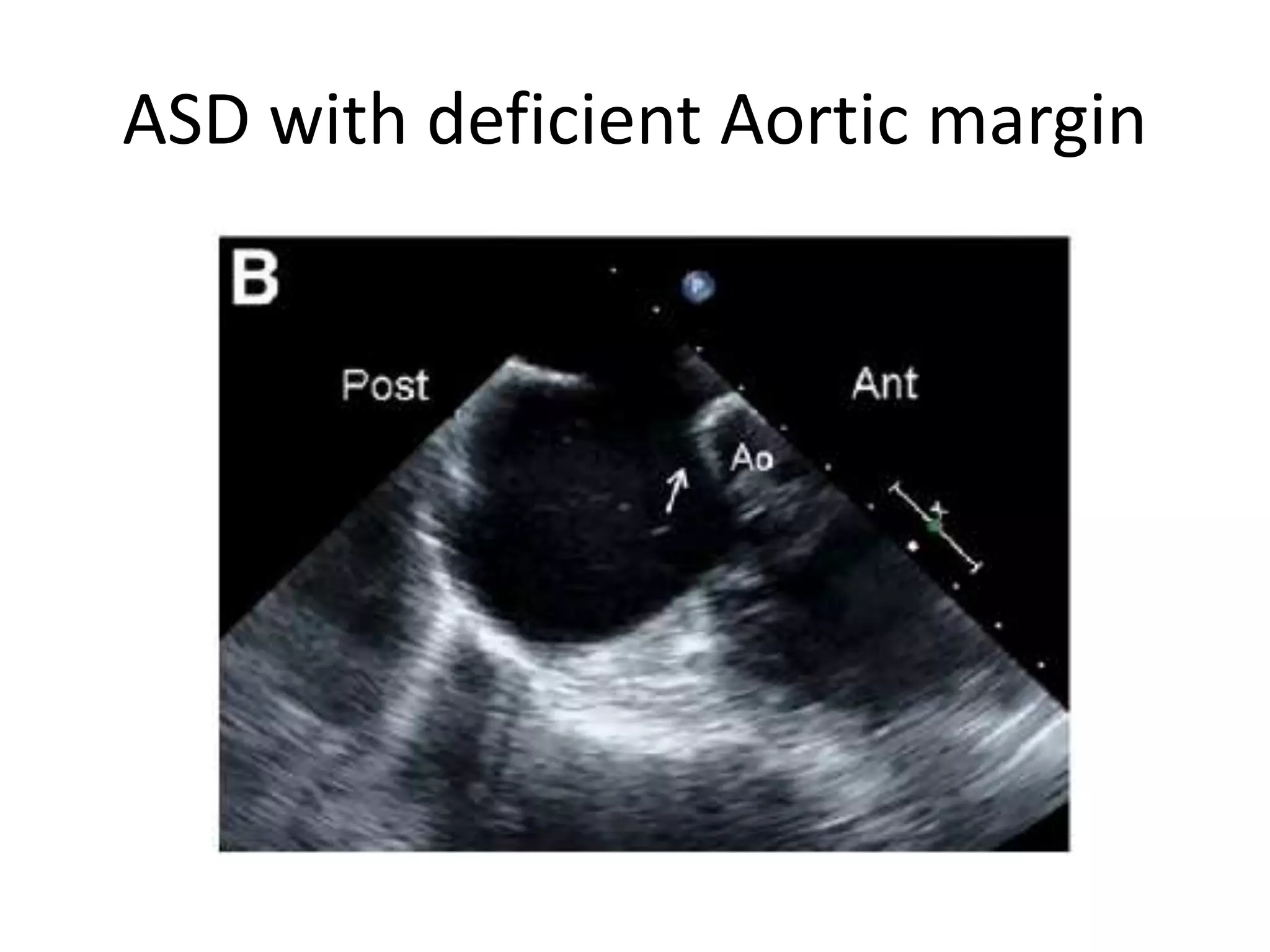
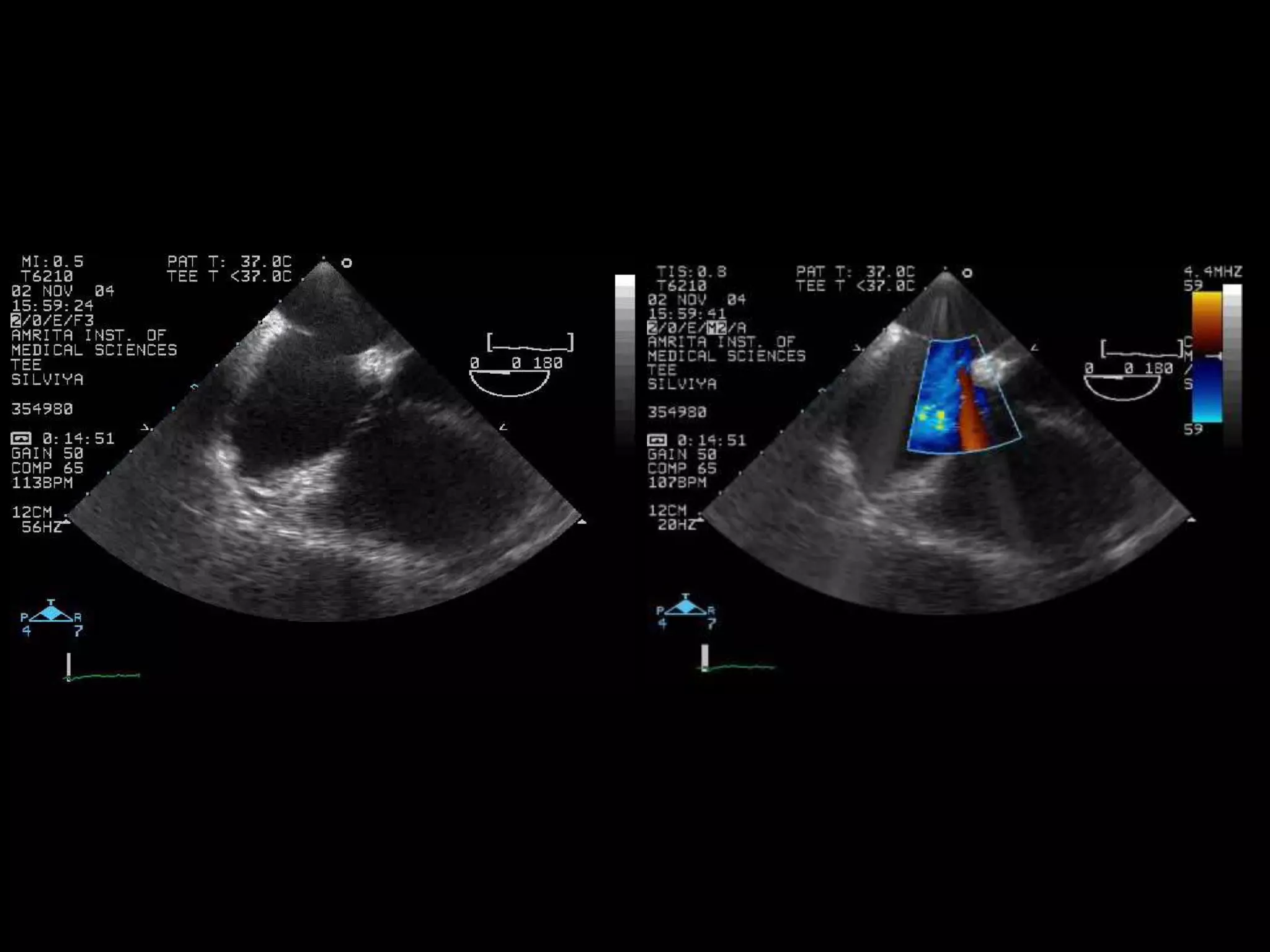
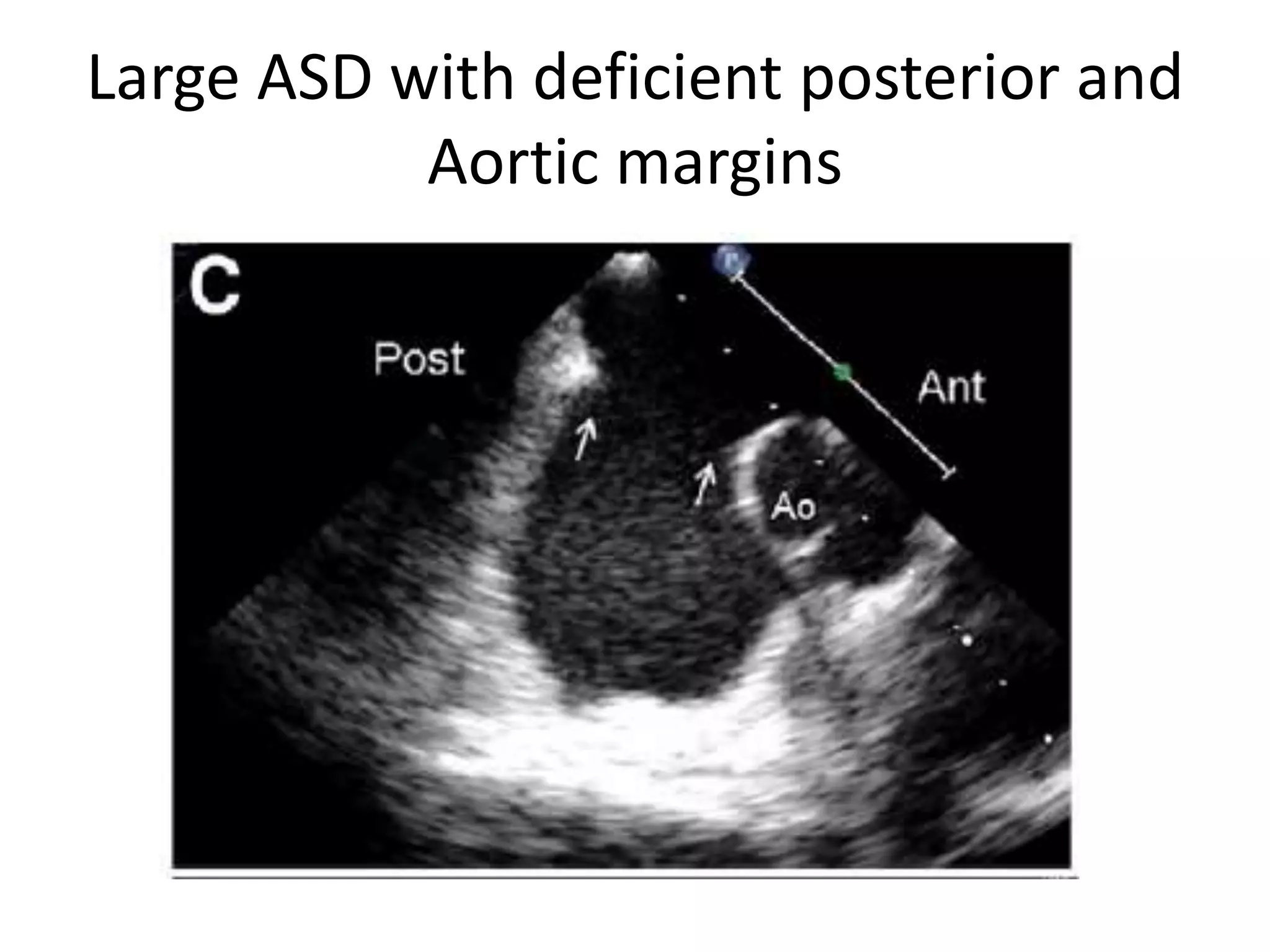
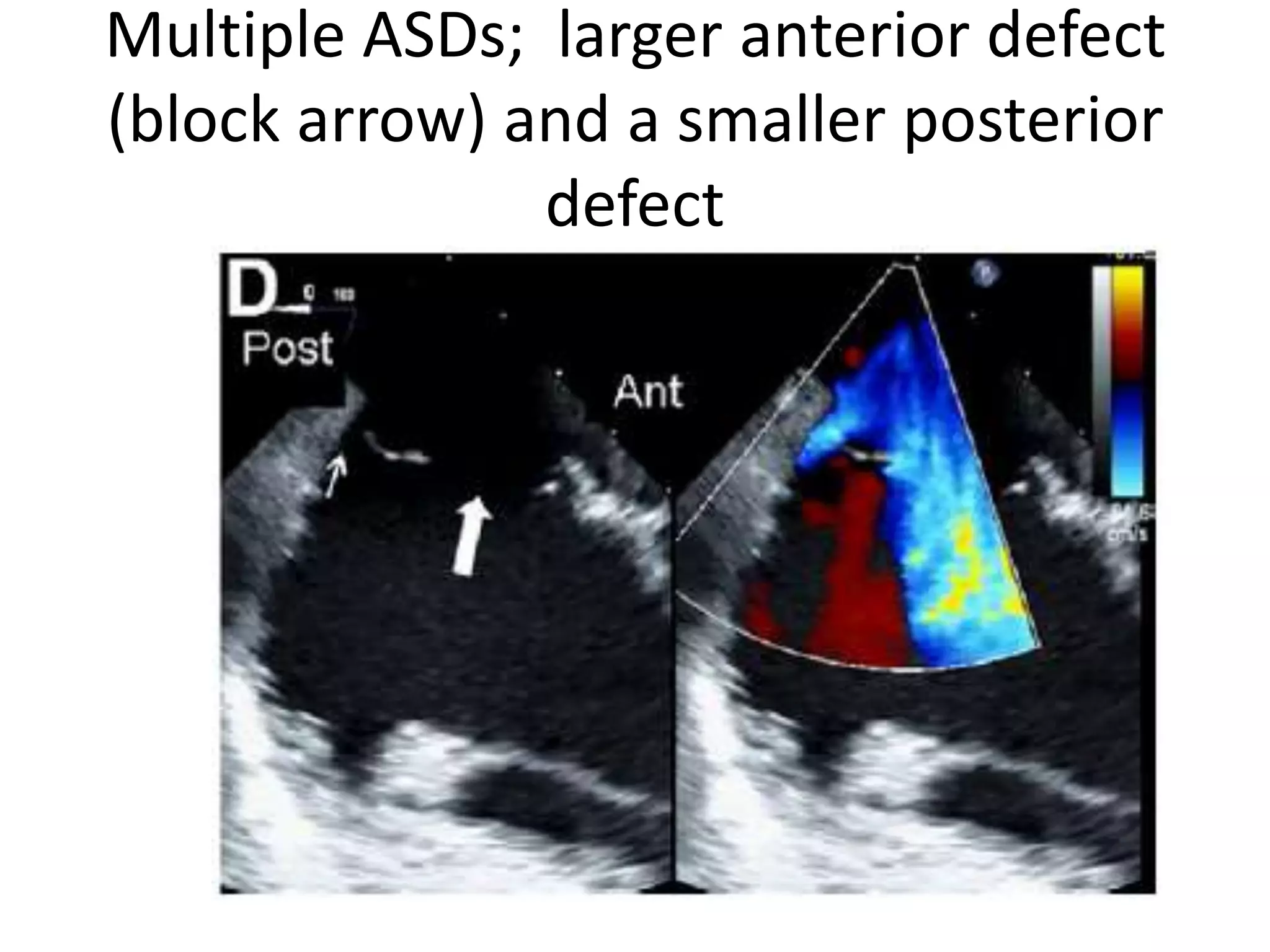
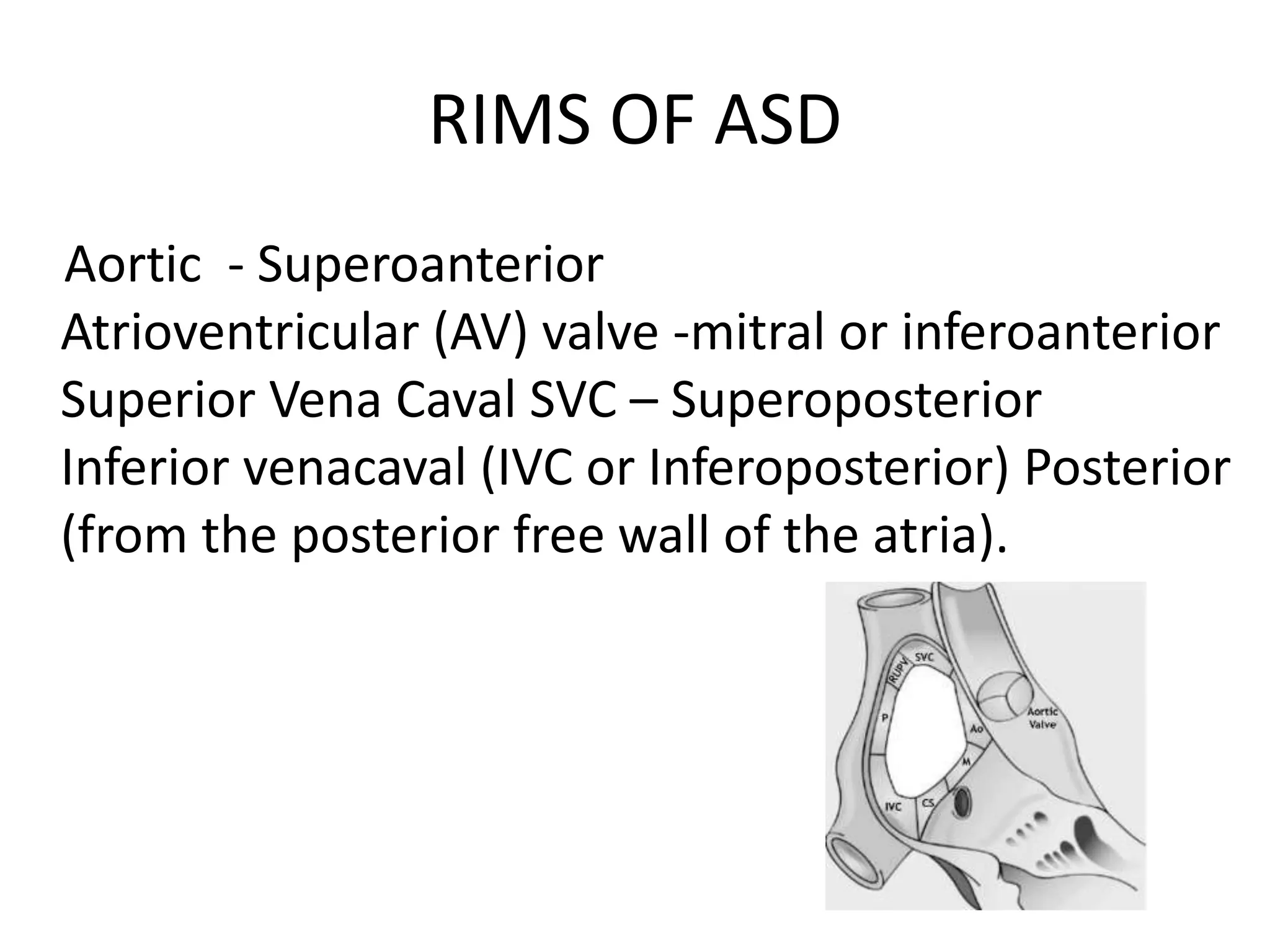
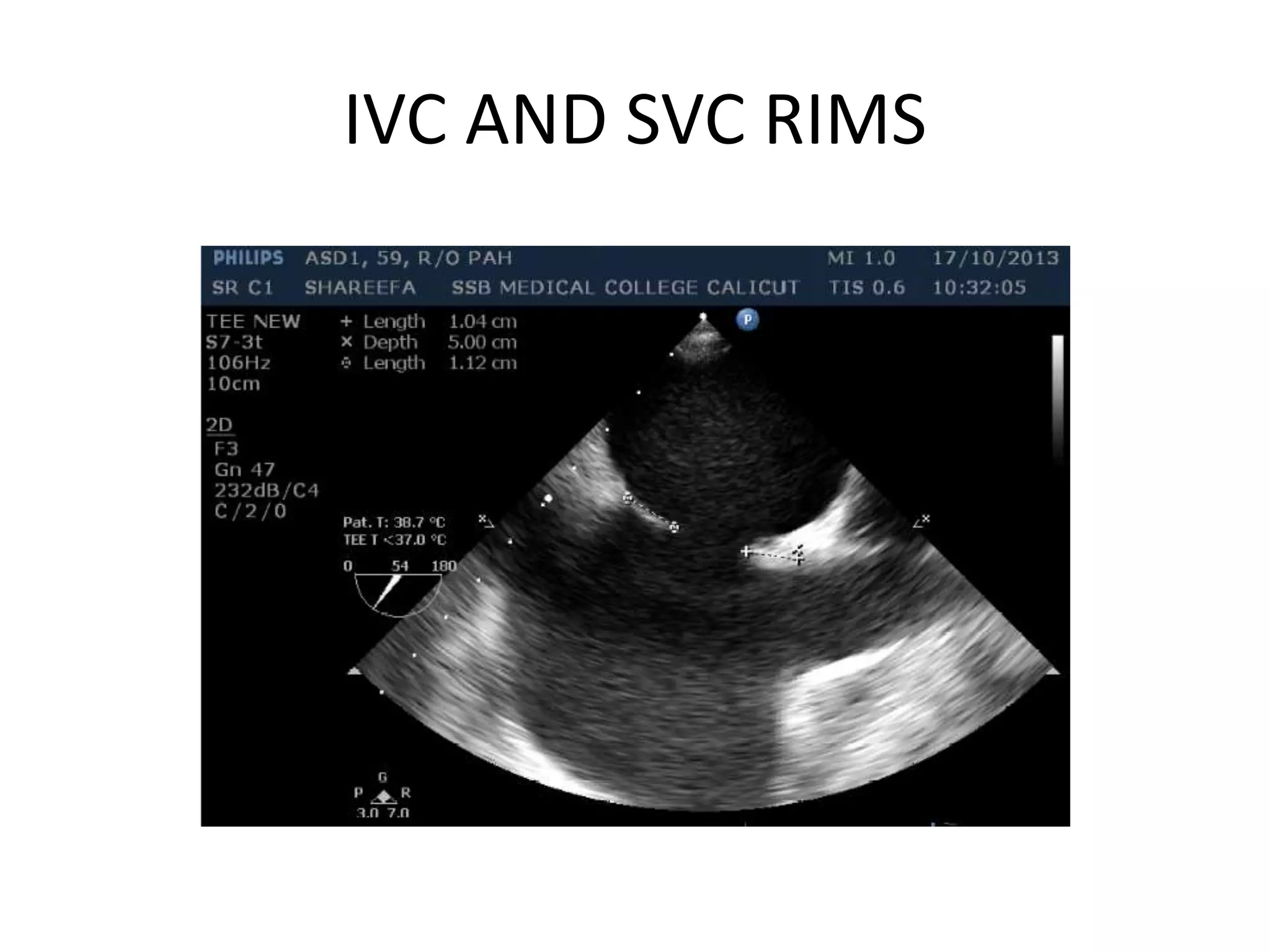
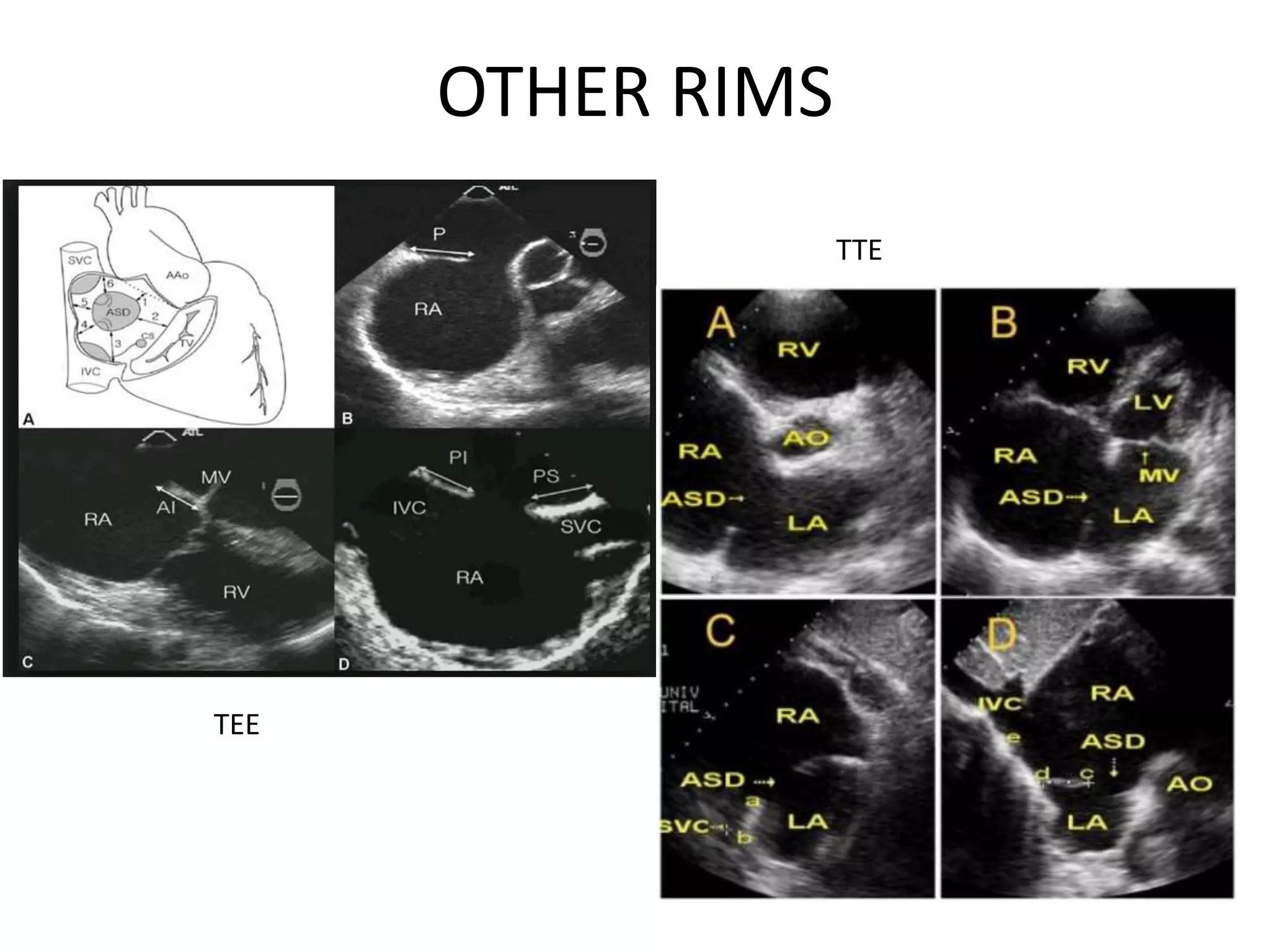
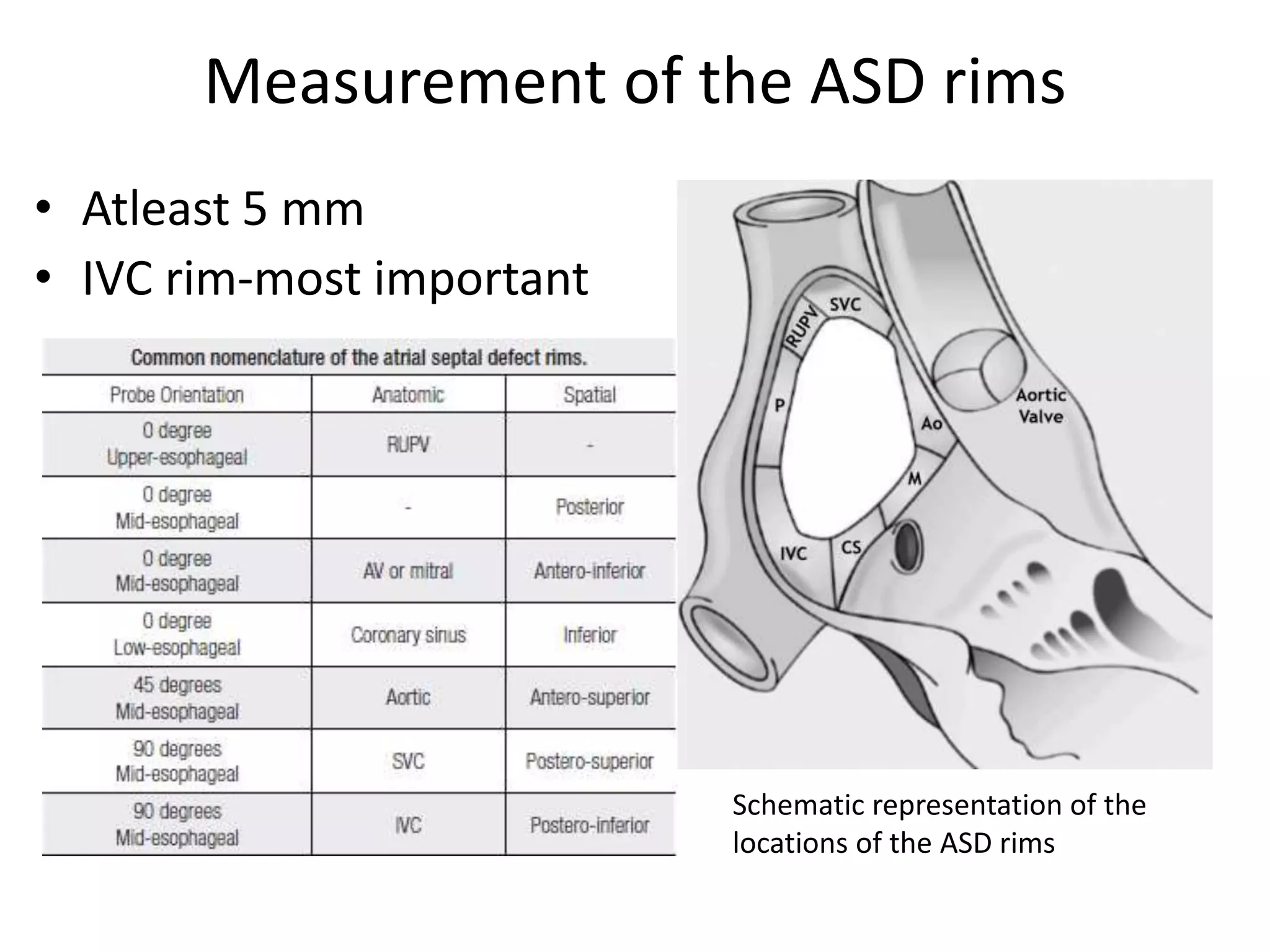
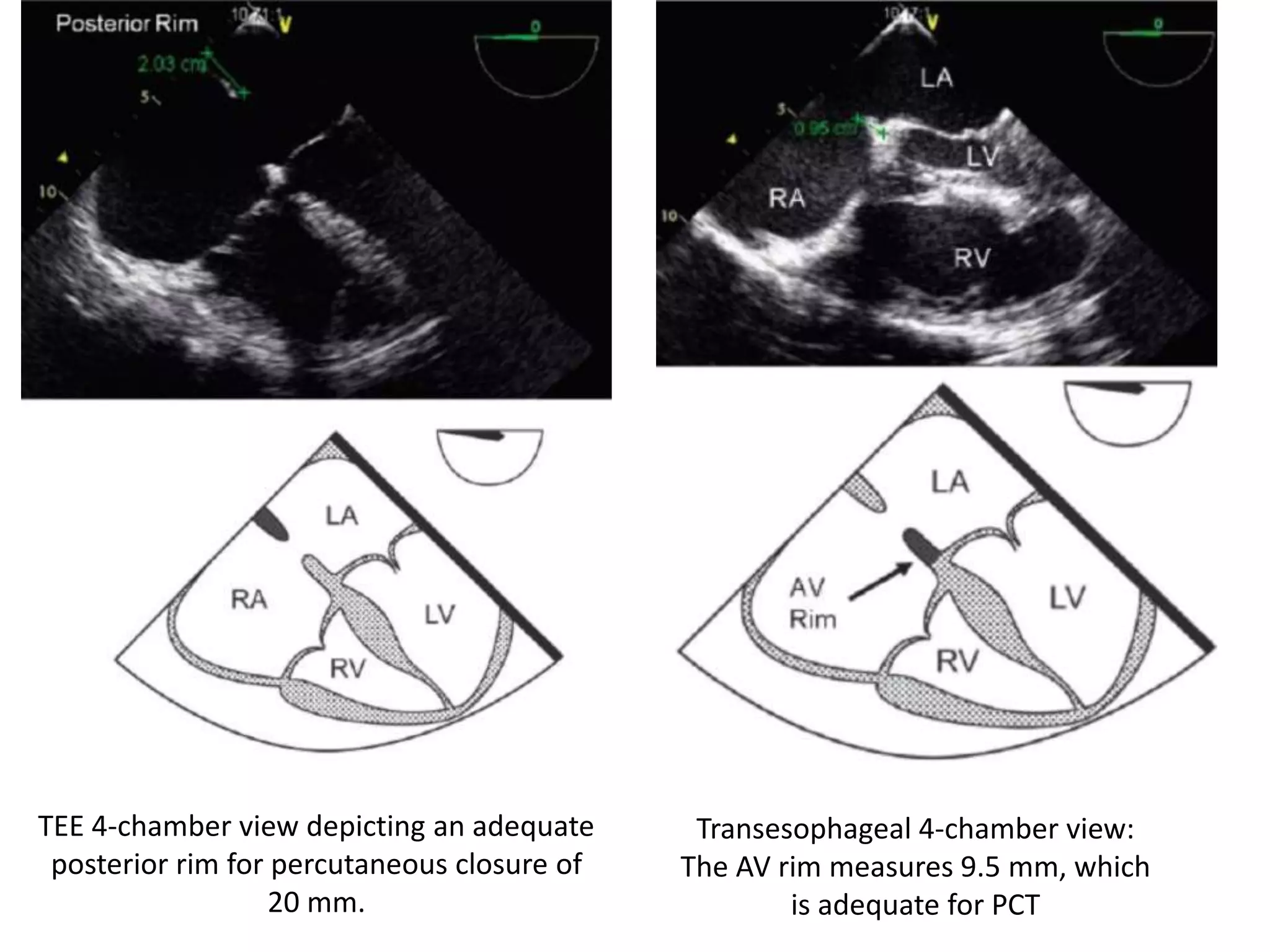
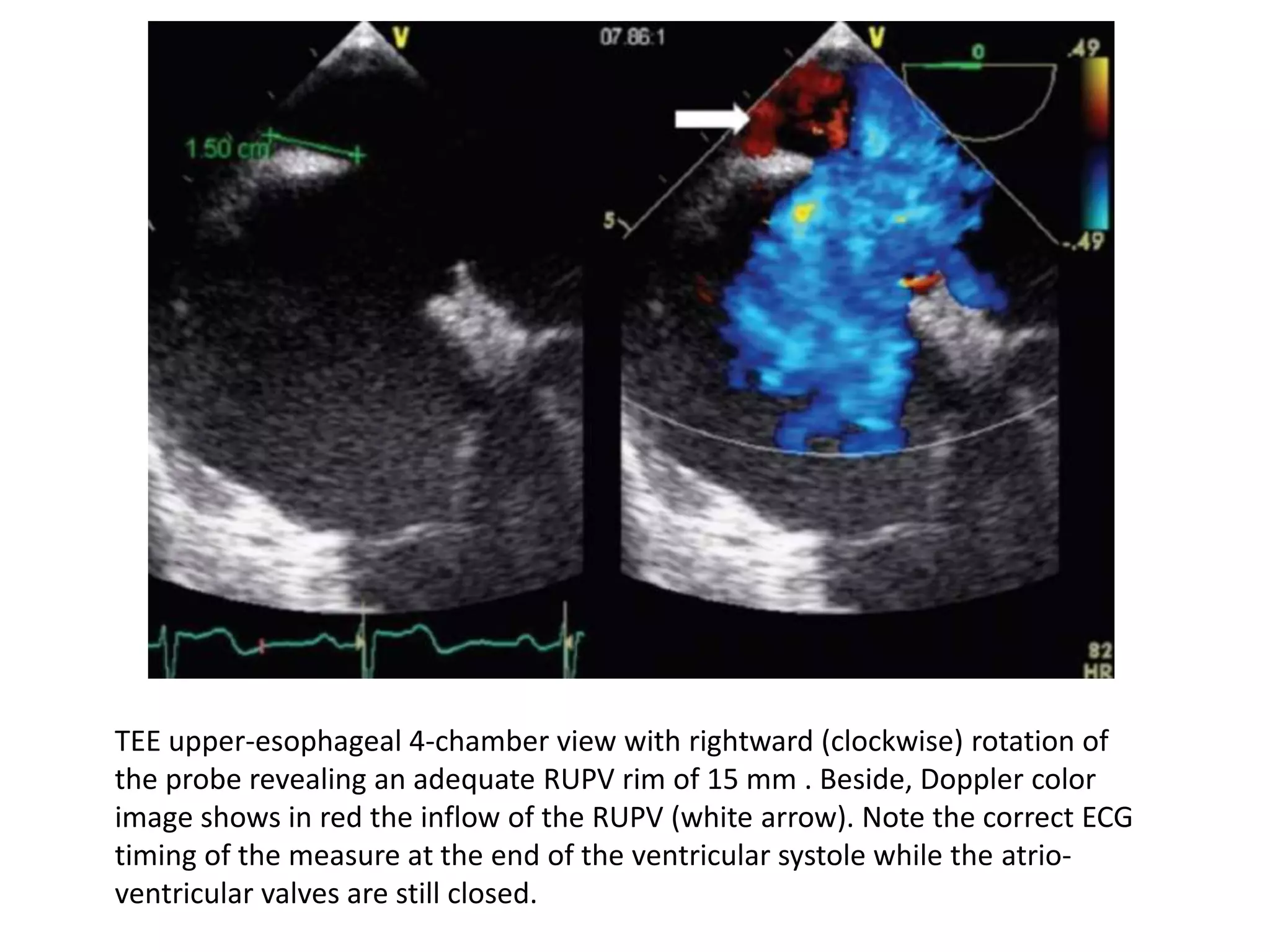
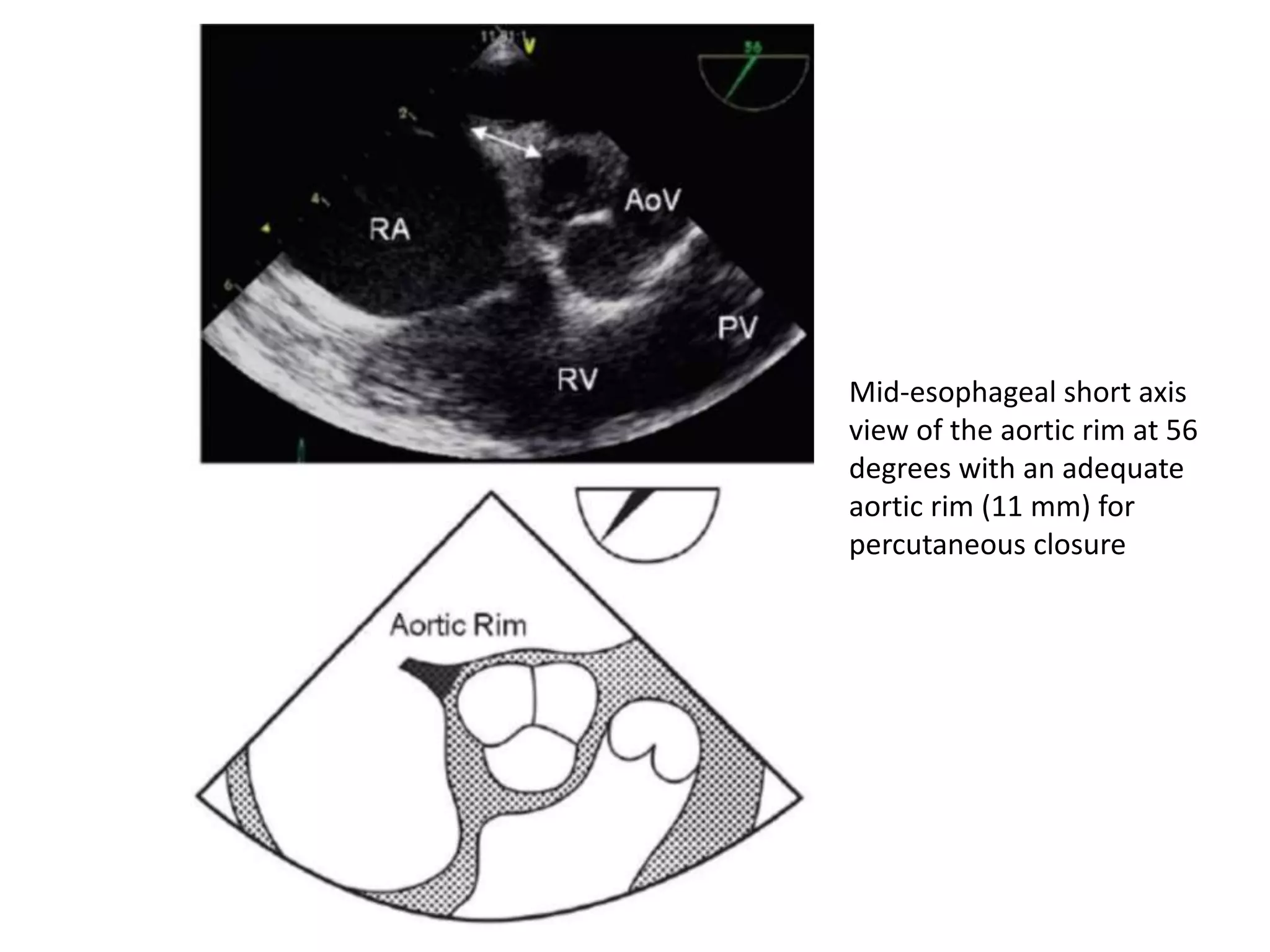
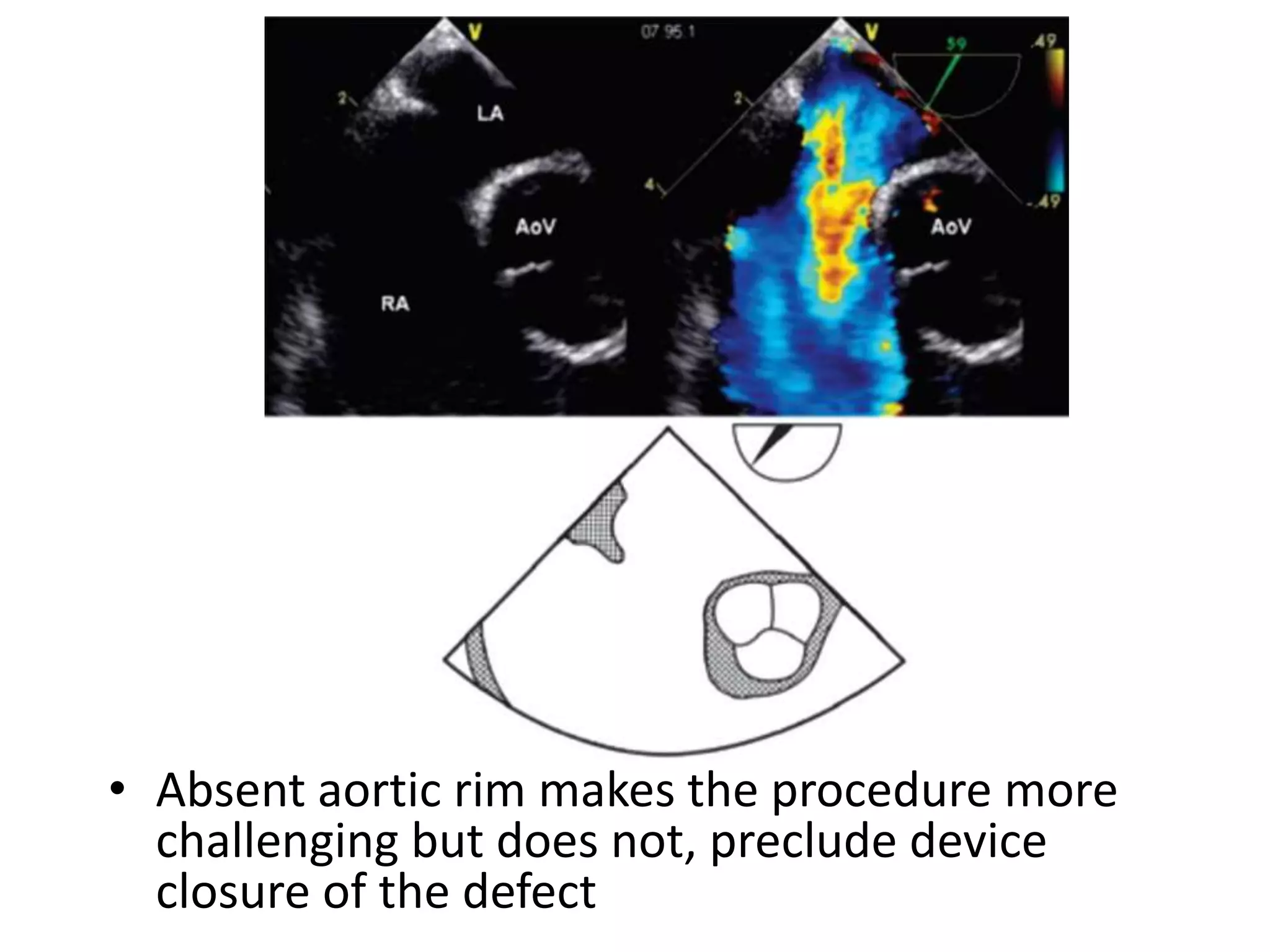
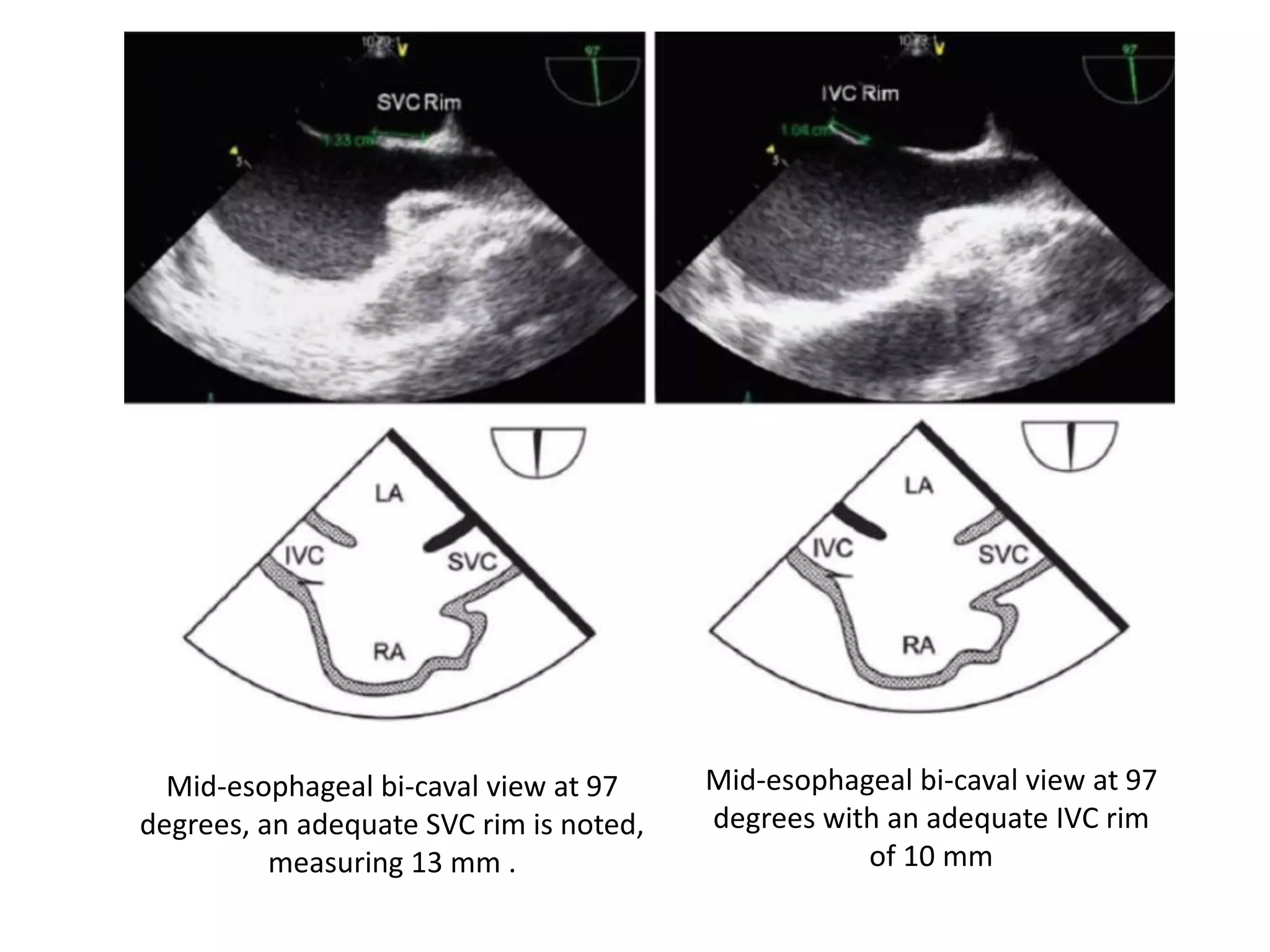
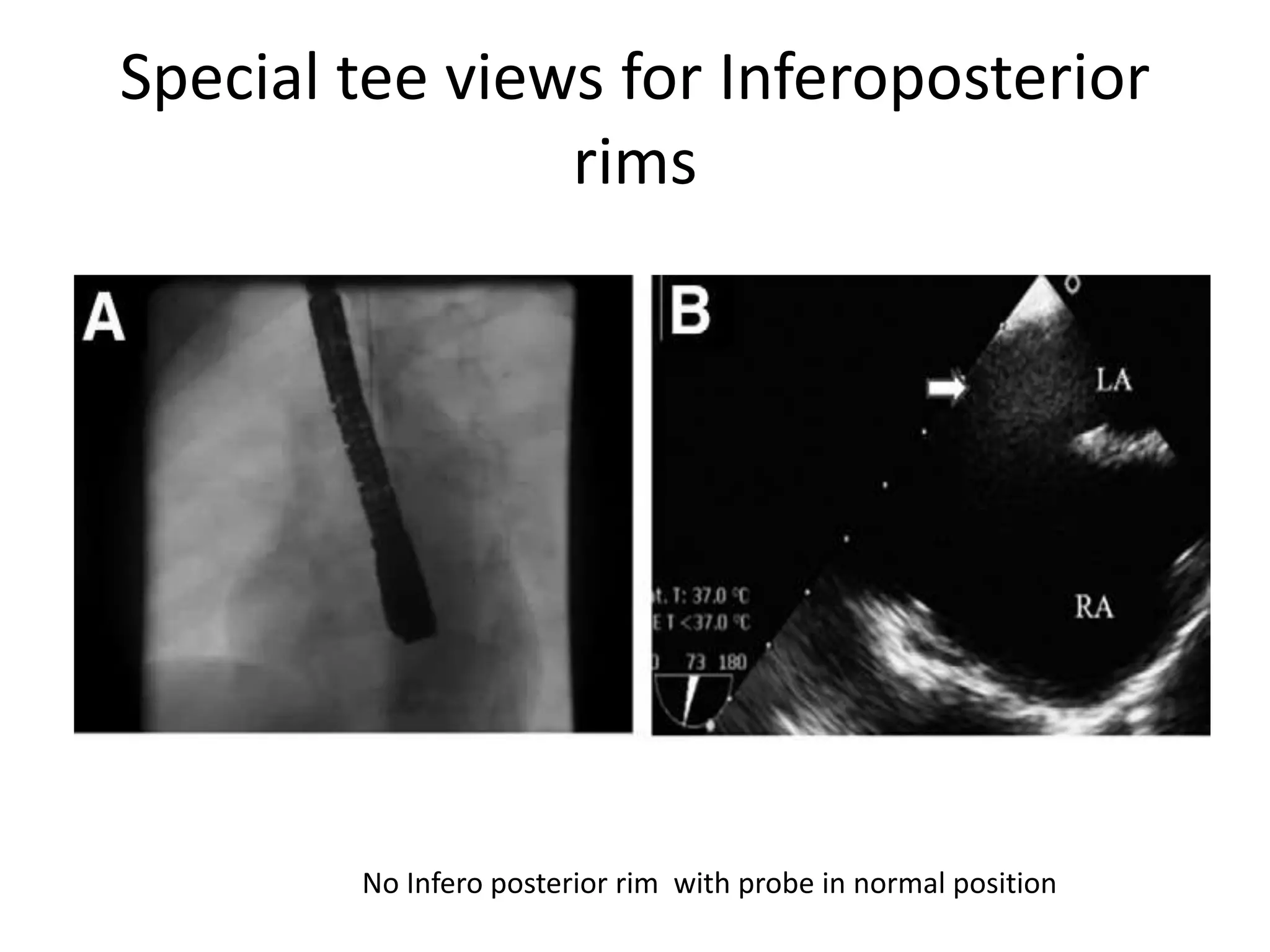
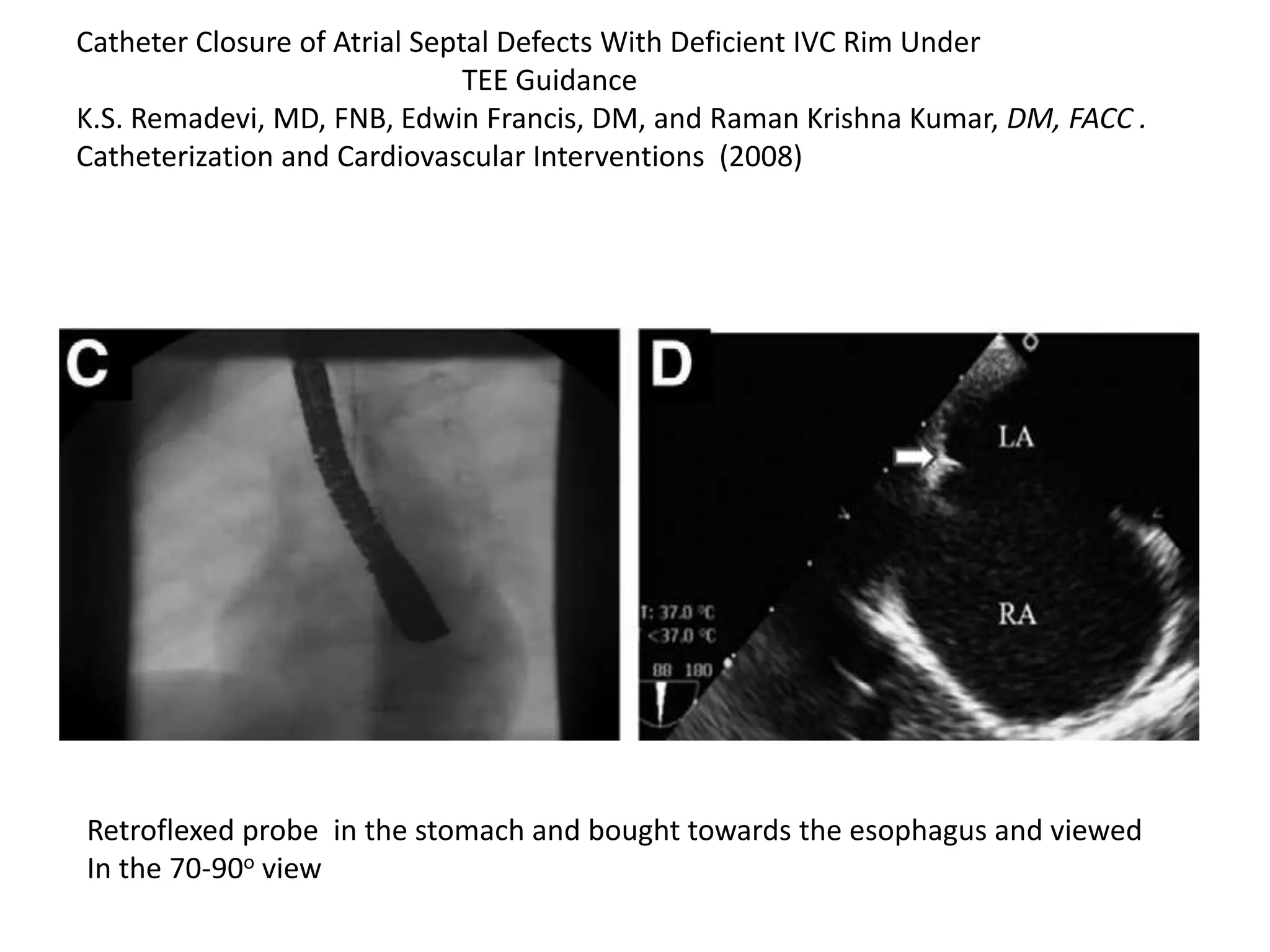
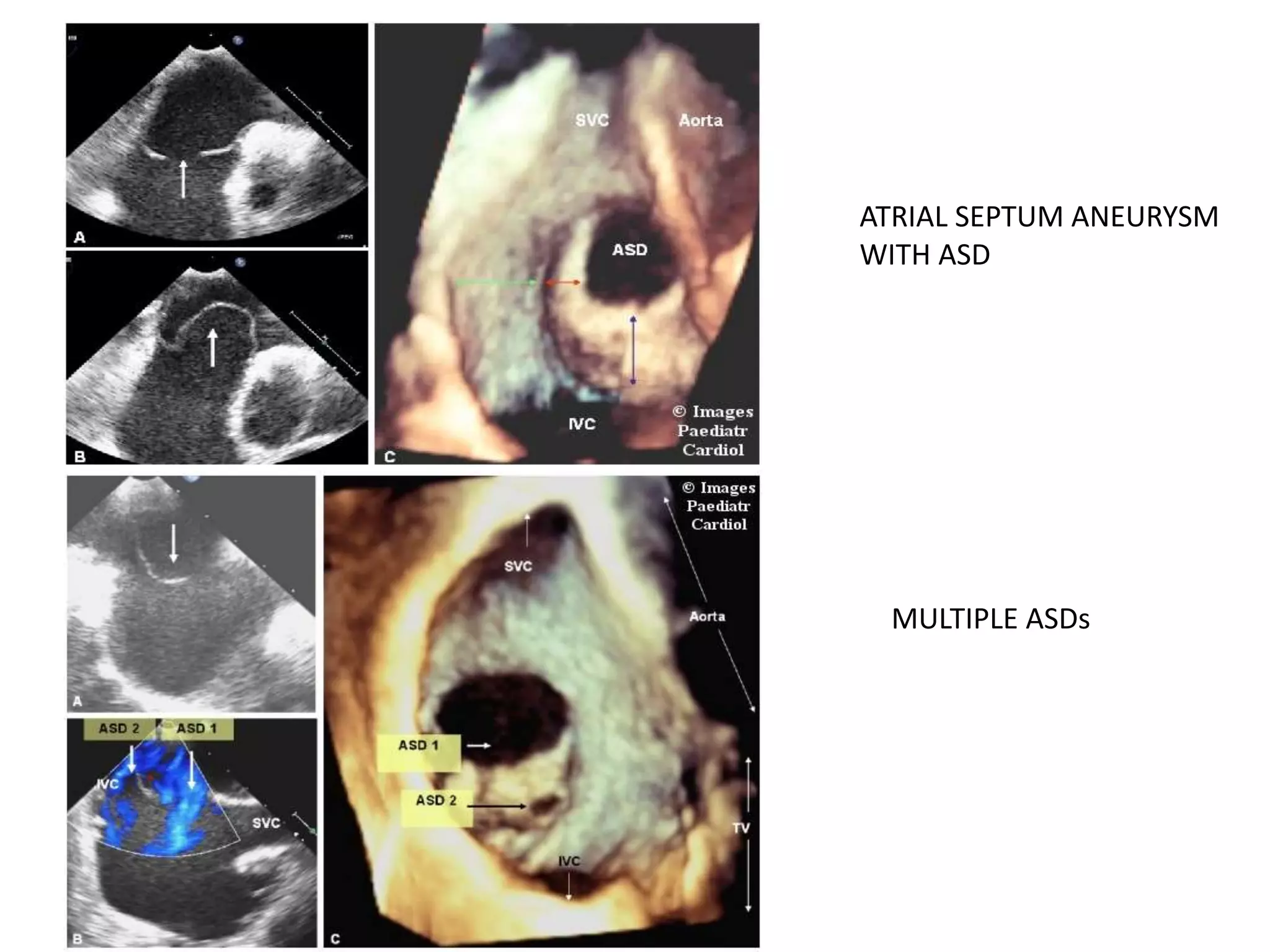
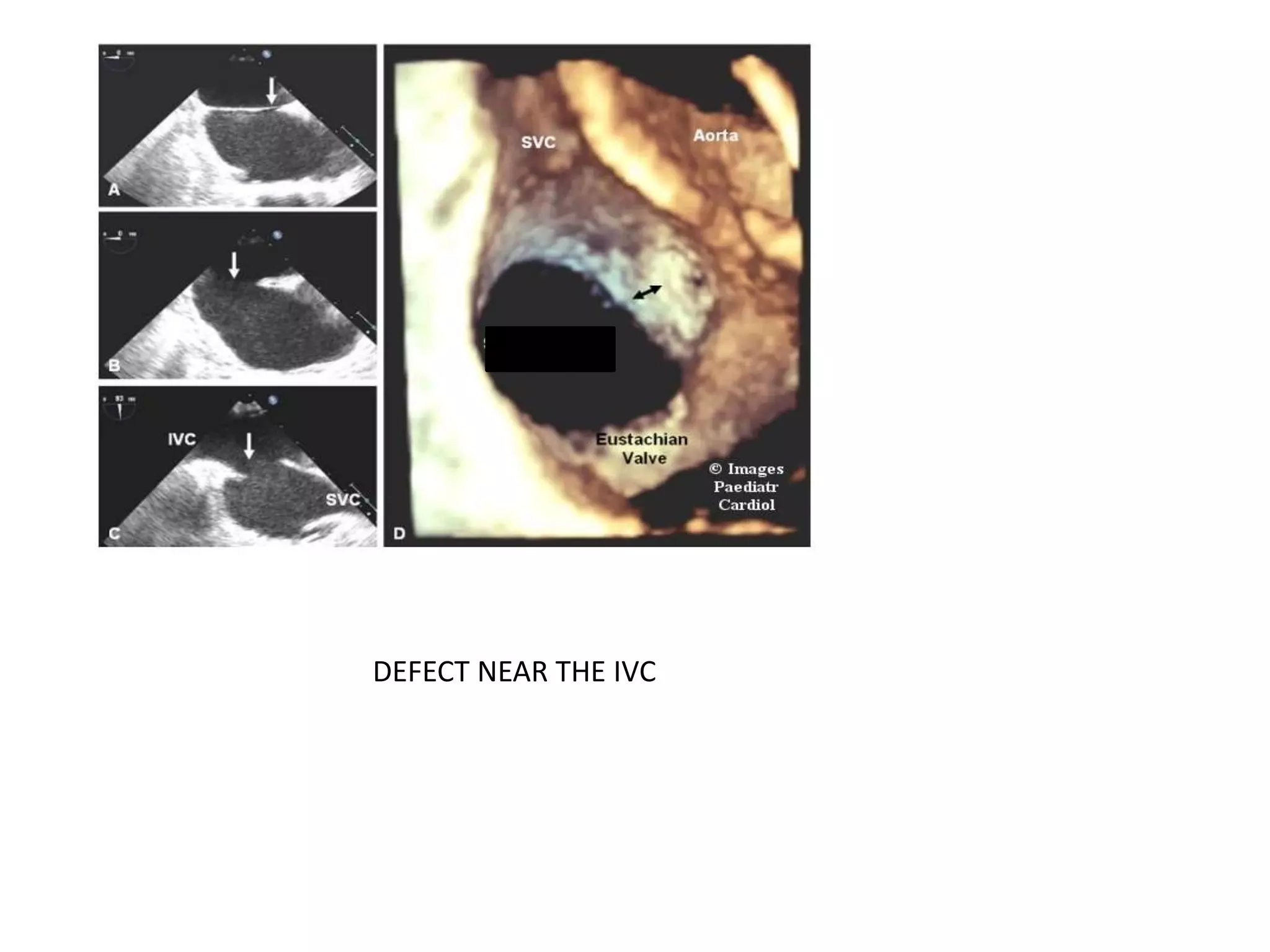
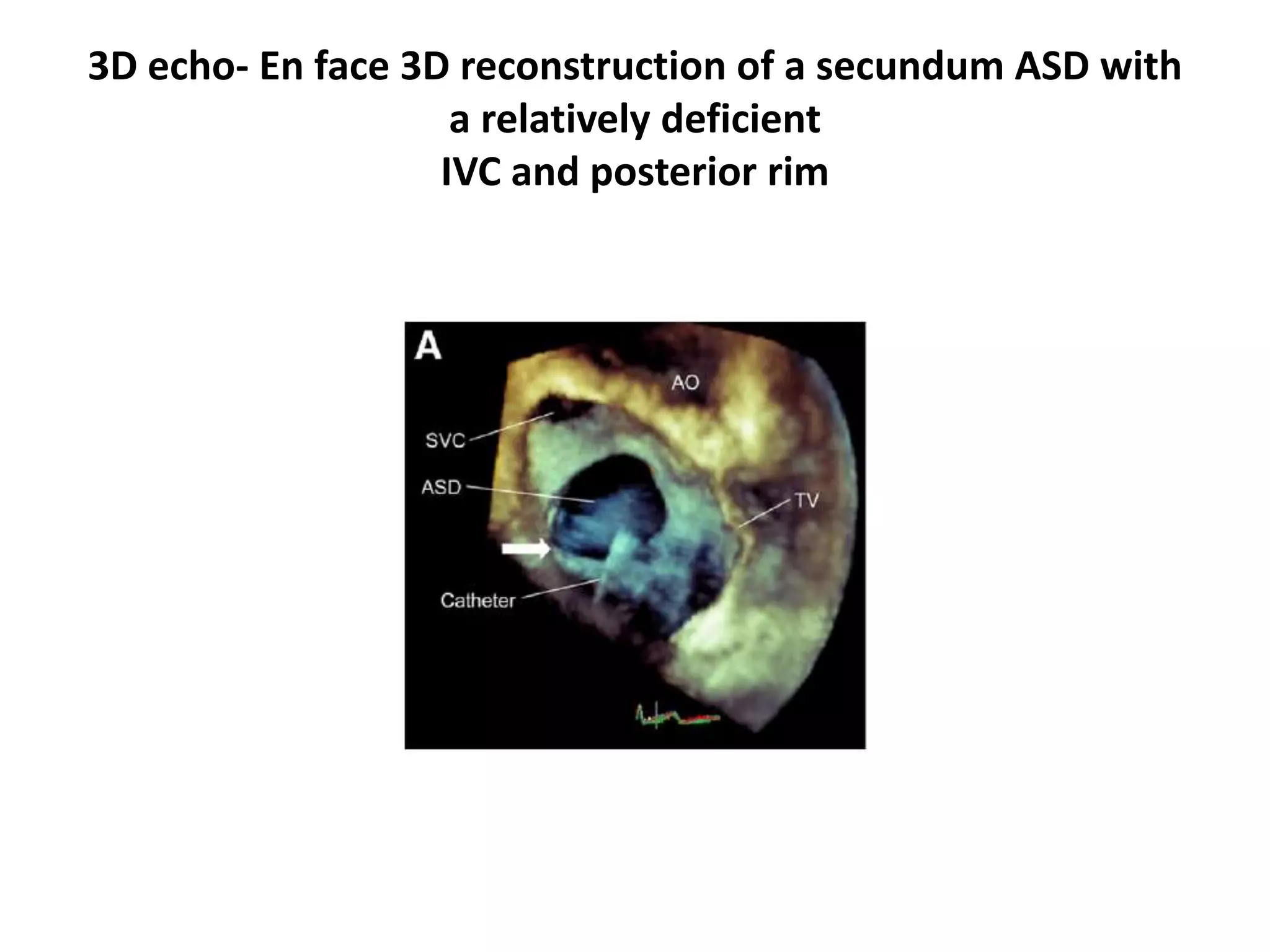
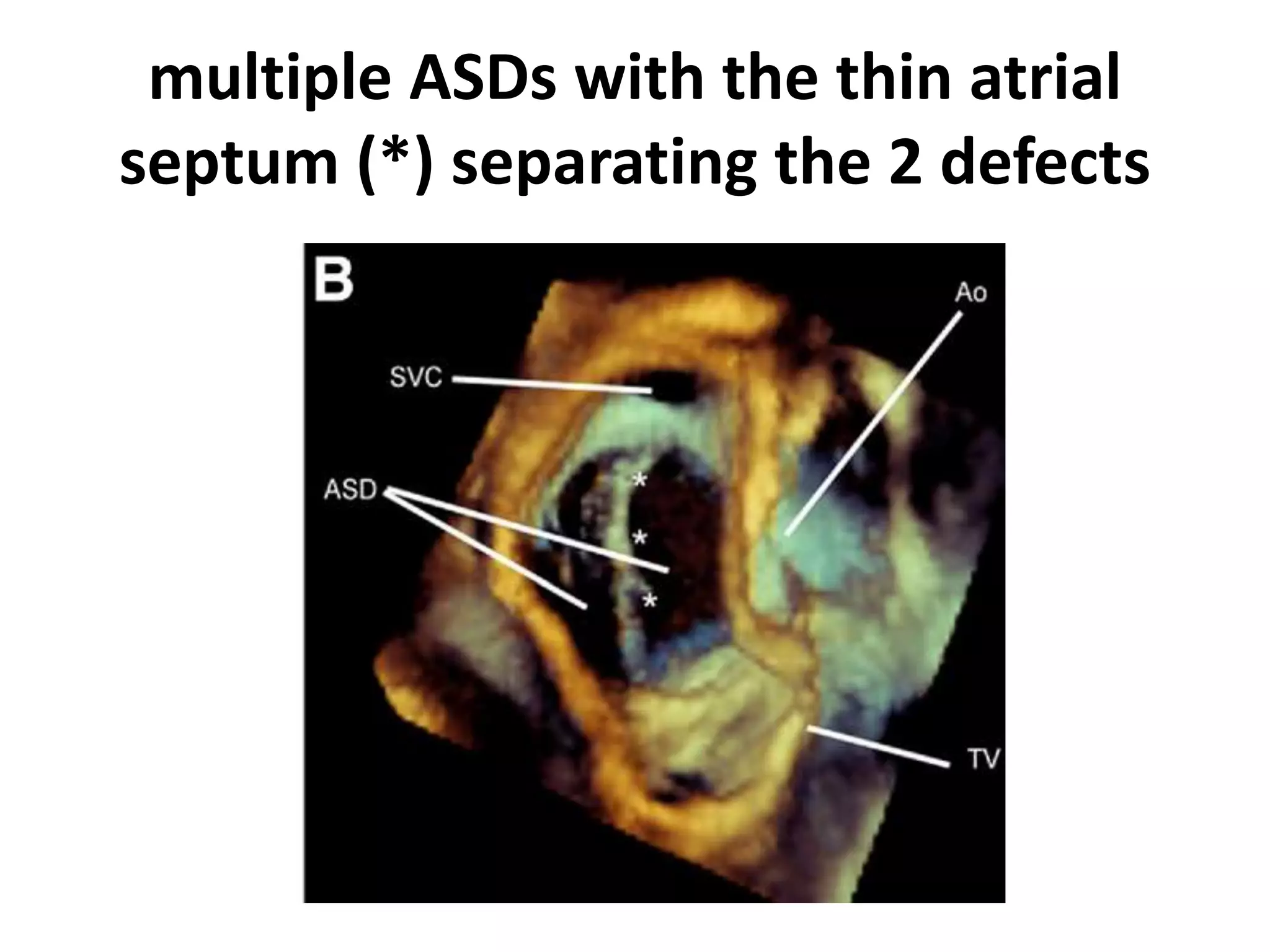
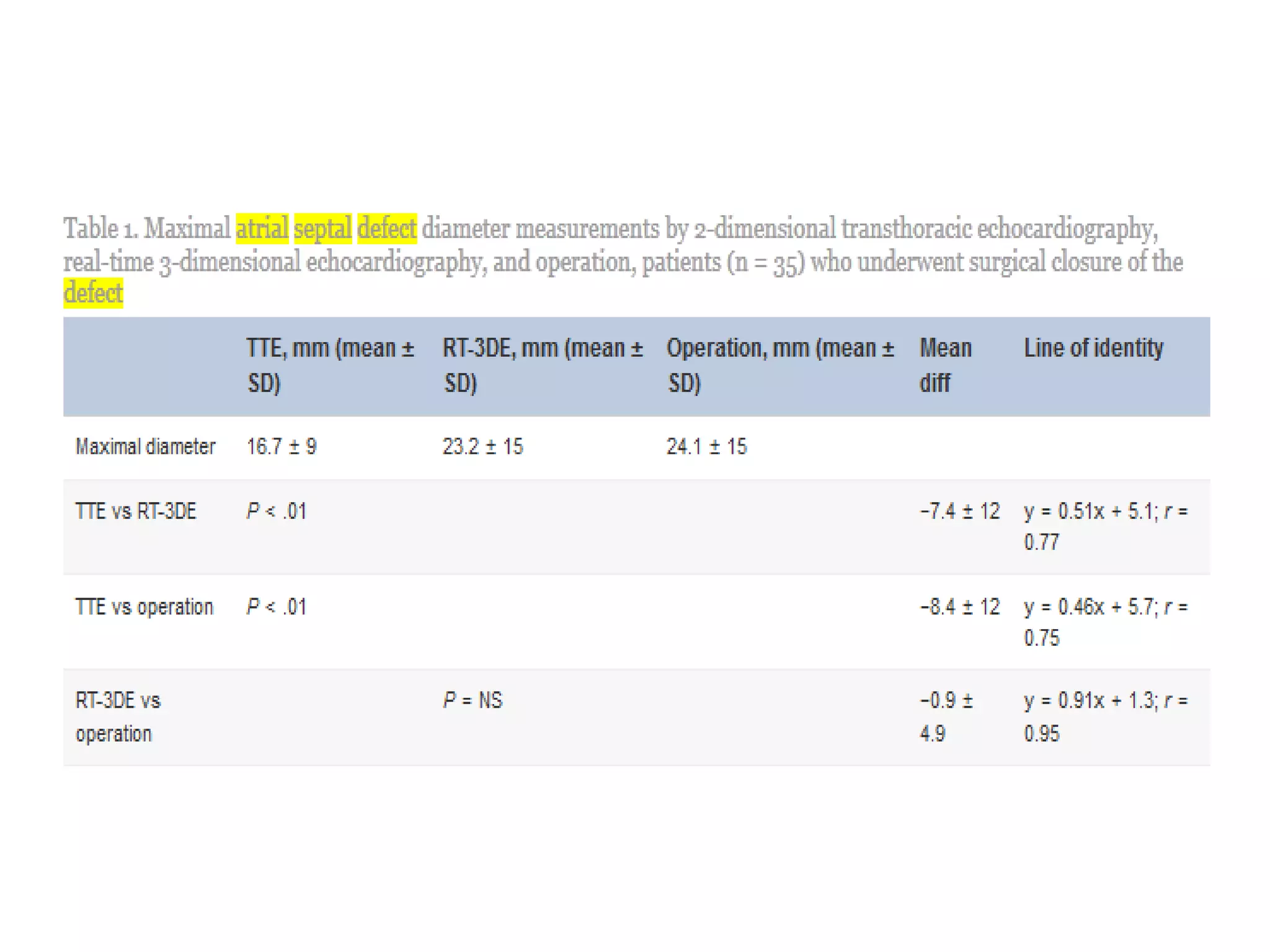
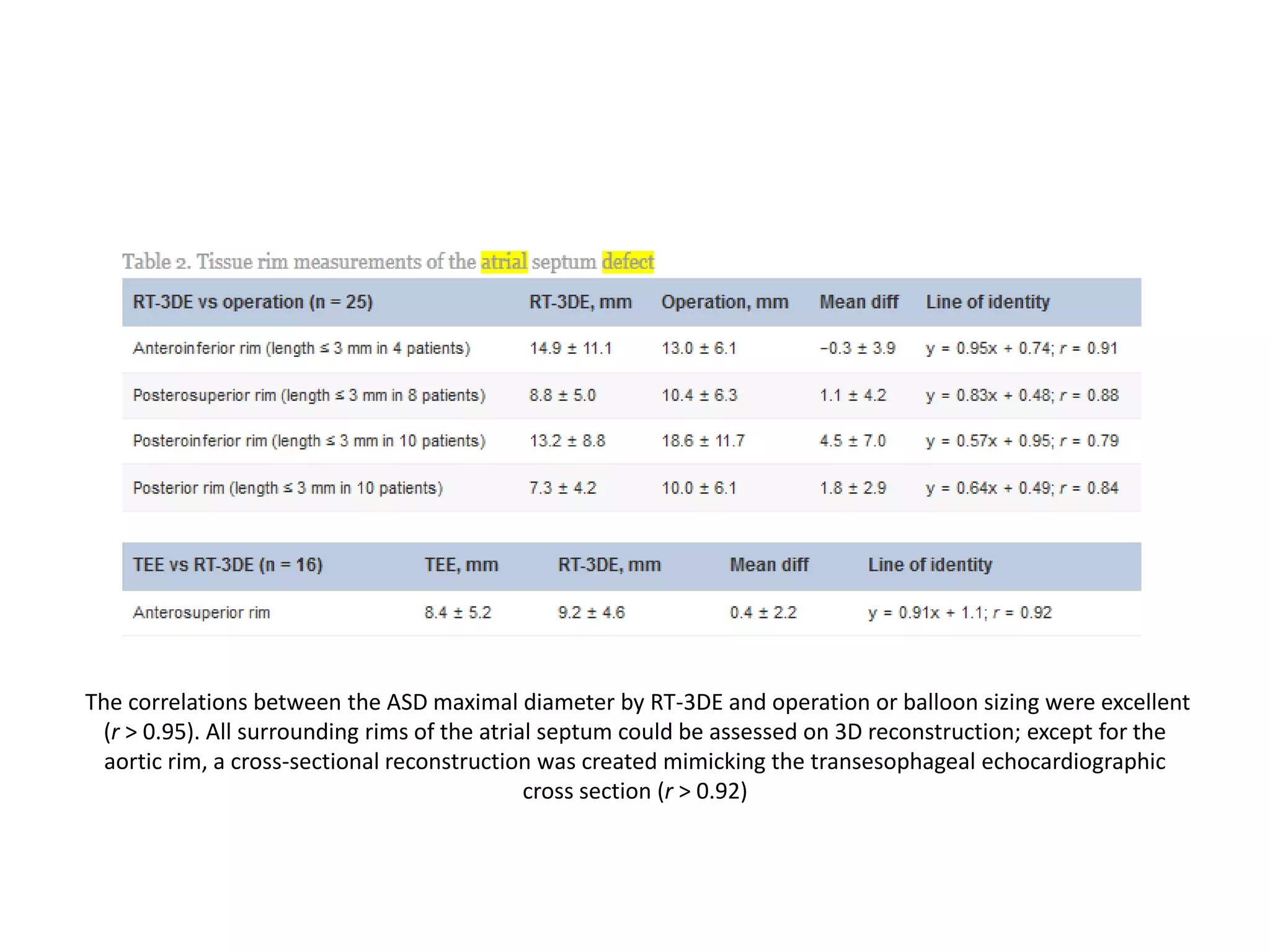
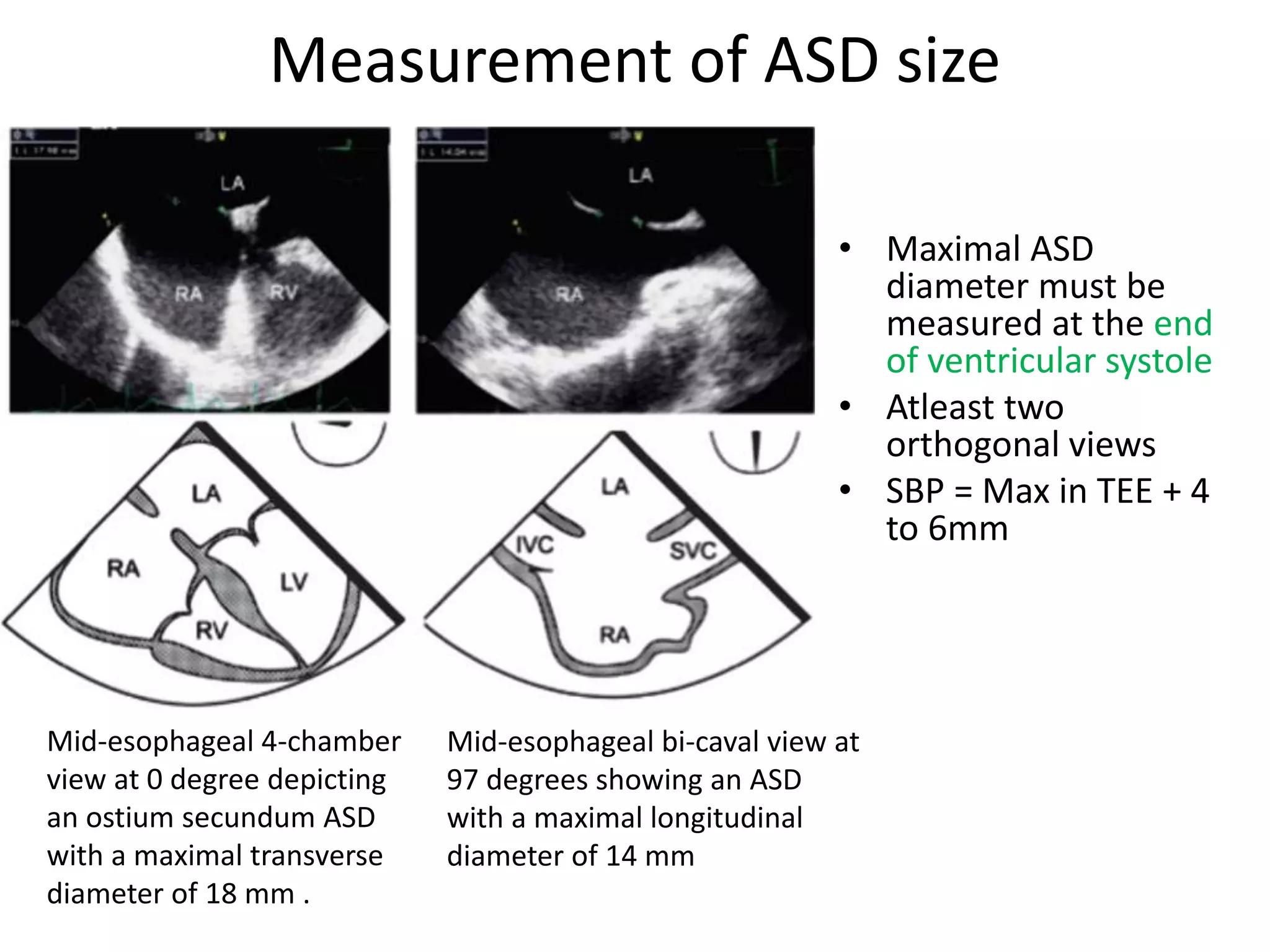

The document provides a comprehensive overview of echocardiographic techniques for assessing atrial septal defects (ASDs), highlighting the importance of various views such as transthoracic echocardiography (TTE) and transesophageal echocardiography (TEE) for accurate diagnosis. It discusses morphological variations of ASDs, criteria for atrial septal aneurysm, and optimal measurement techniques critical for device closure. The conclusion emphasizes the necessity of proper case selection to ensure successful percutaneous closure, focusing on the requirement of sufficient inferior and posterior rims.