Downloaded 533 times





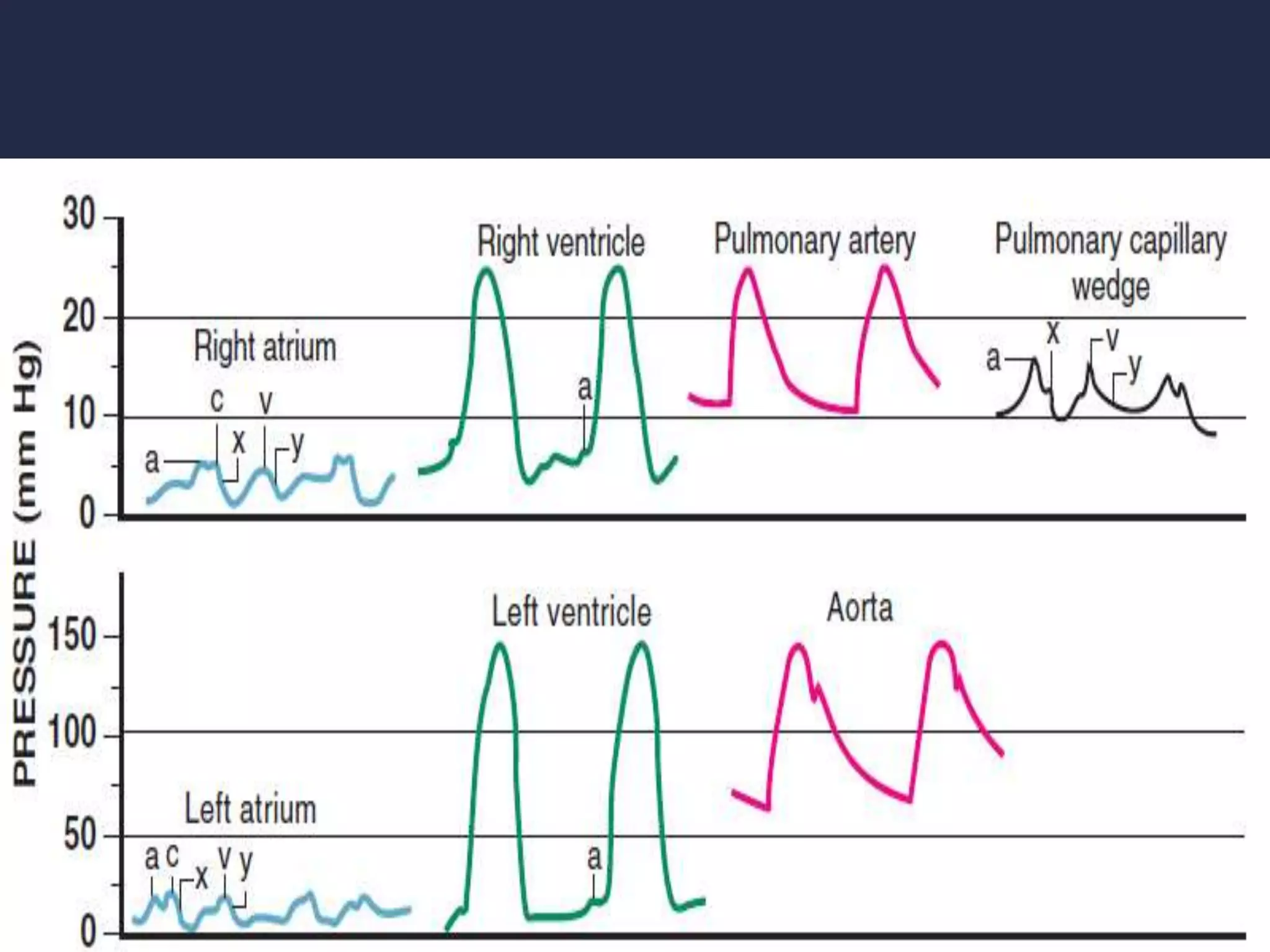


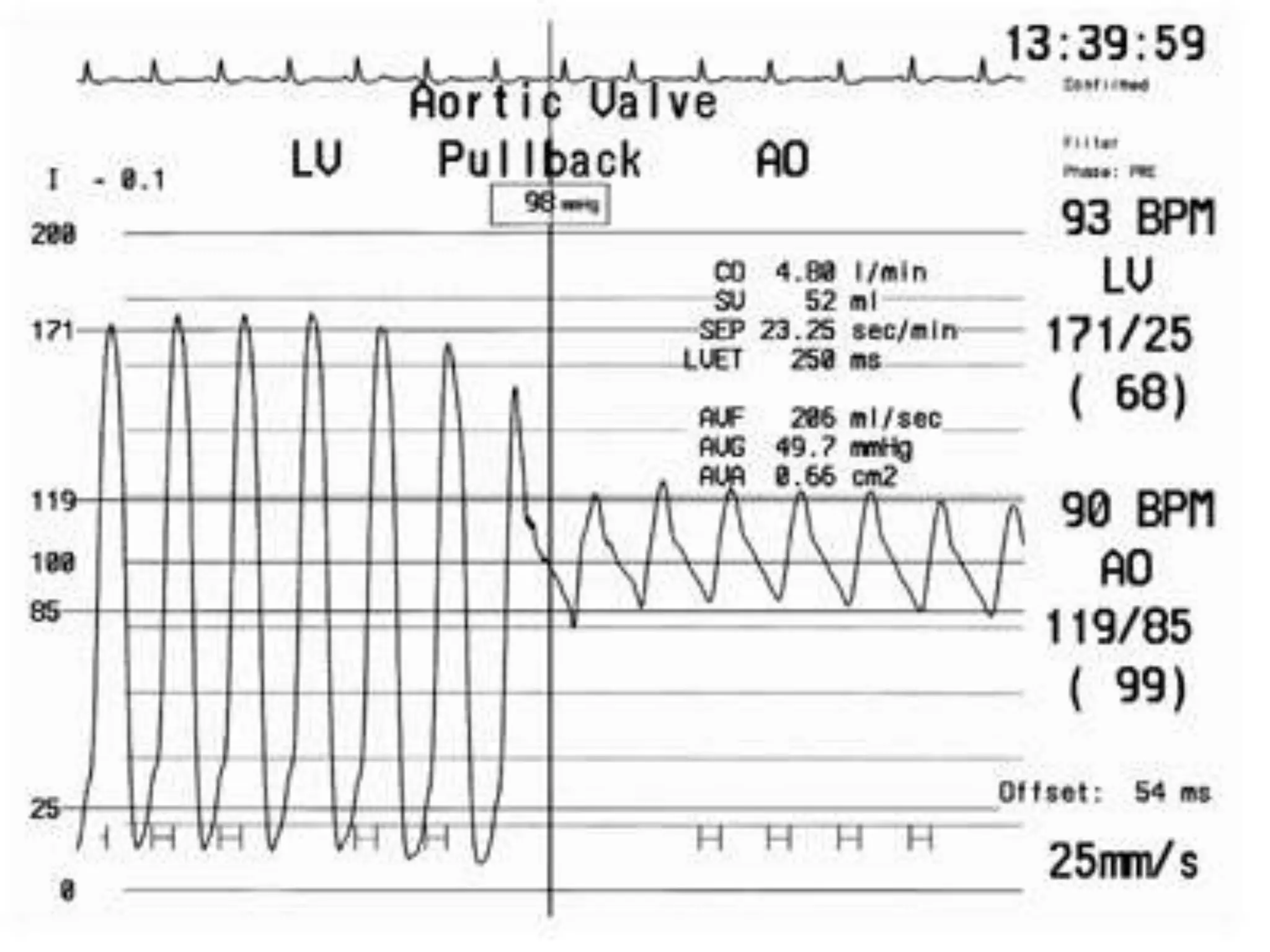
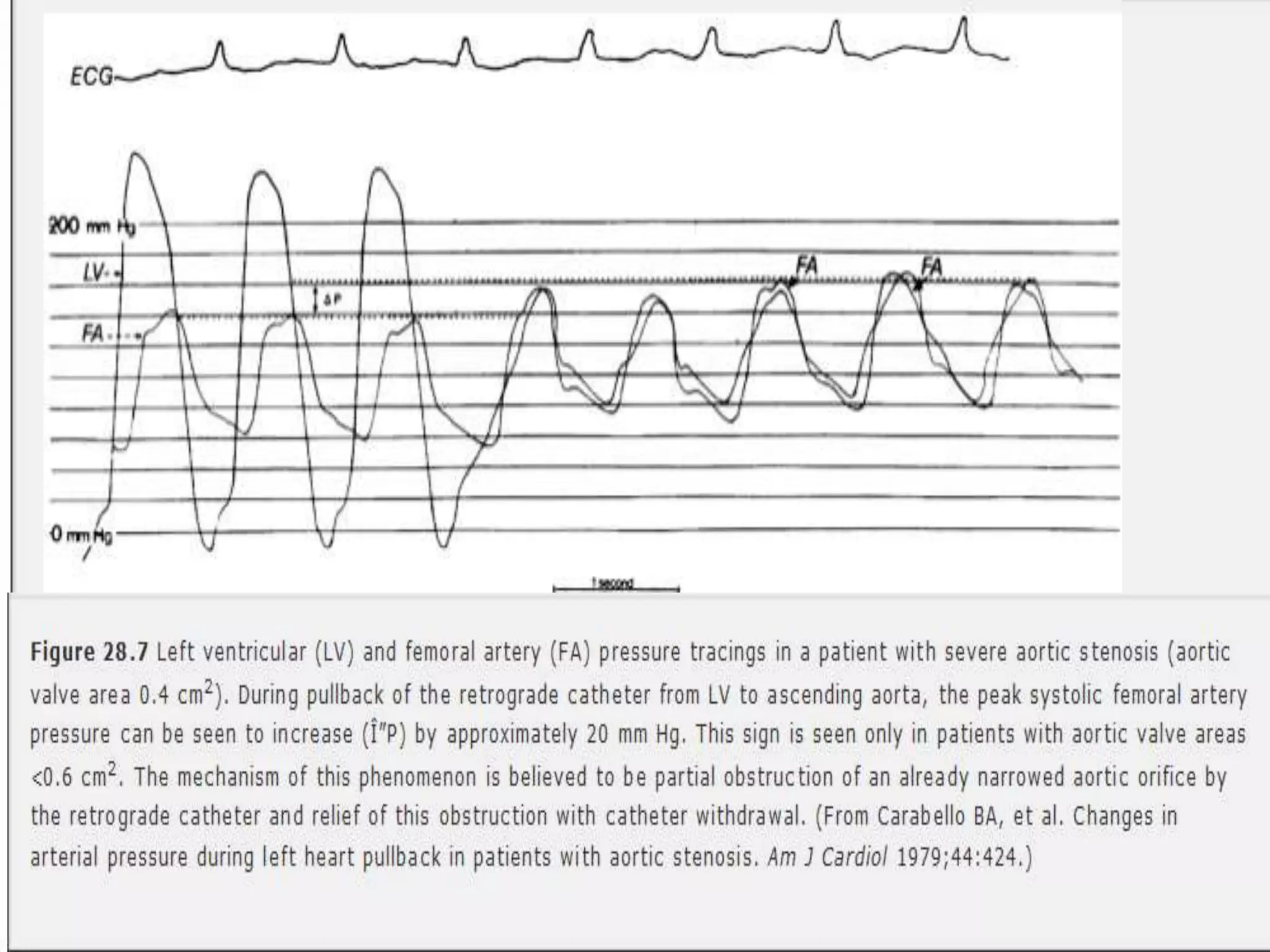
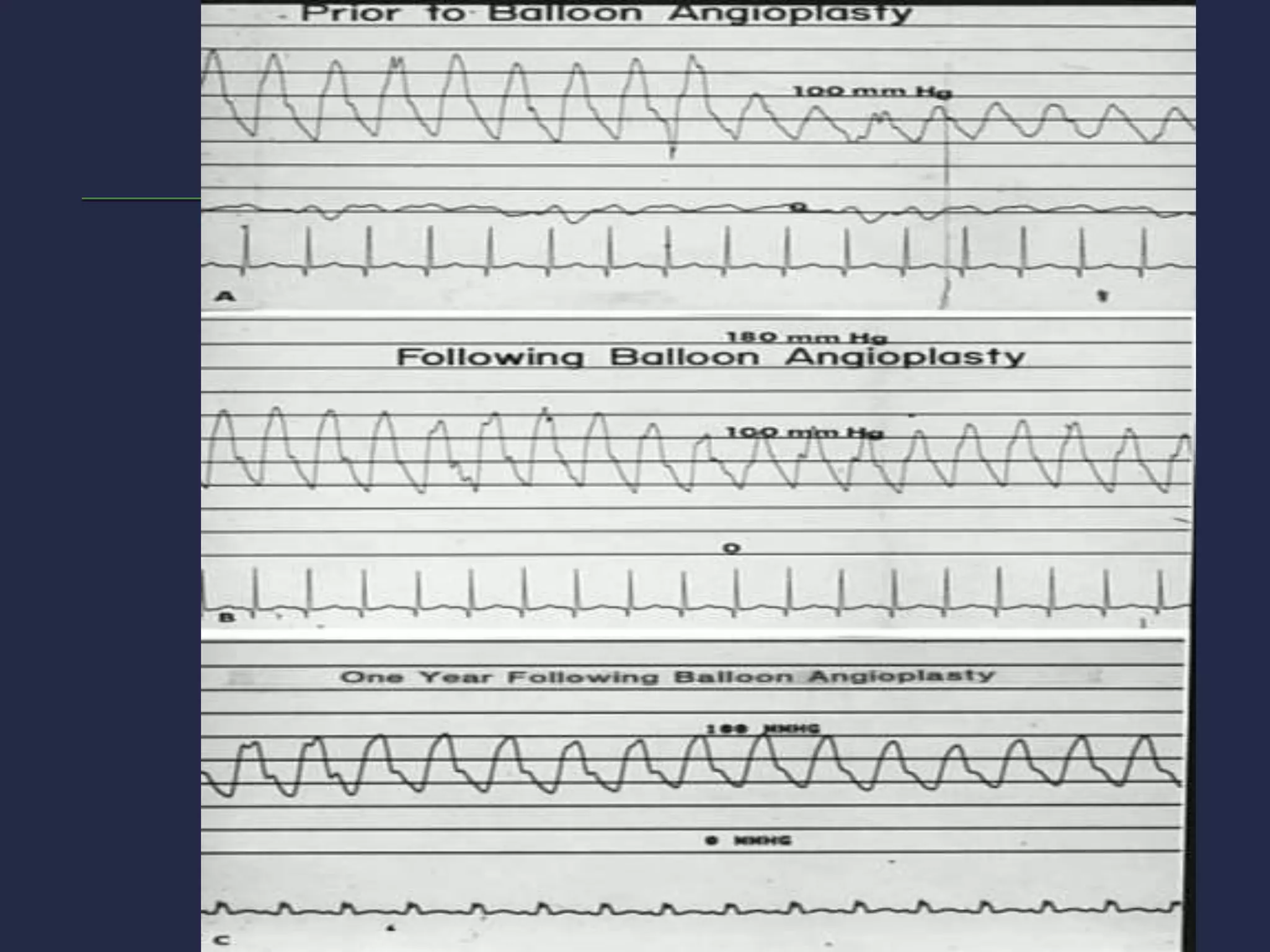



This document provides an overview of cardiac catheterization procedures. It discusses indications, contraindications, techniques, views obtained, and interpretation of pressure waveforms. Key points include that cardiac catheterization guides treatment decisions by measuring pressures, outputs, and obtaining images. It is now often used therapeutically for procedures like angioplasty and device closures. The document outlines patient preparation, access methods, catheters used, views obtained, and complications that can occur.























































































