Downloaded 965 times






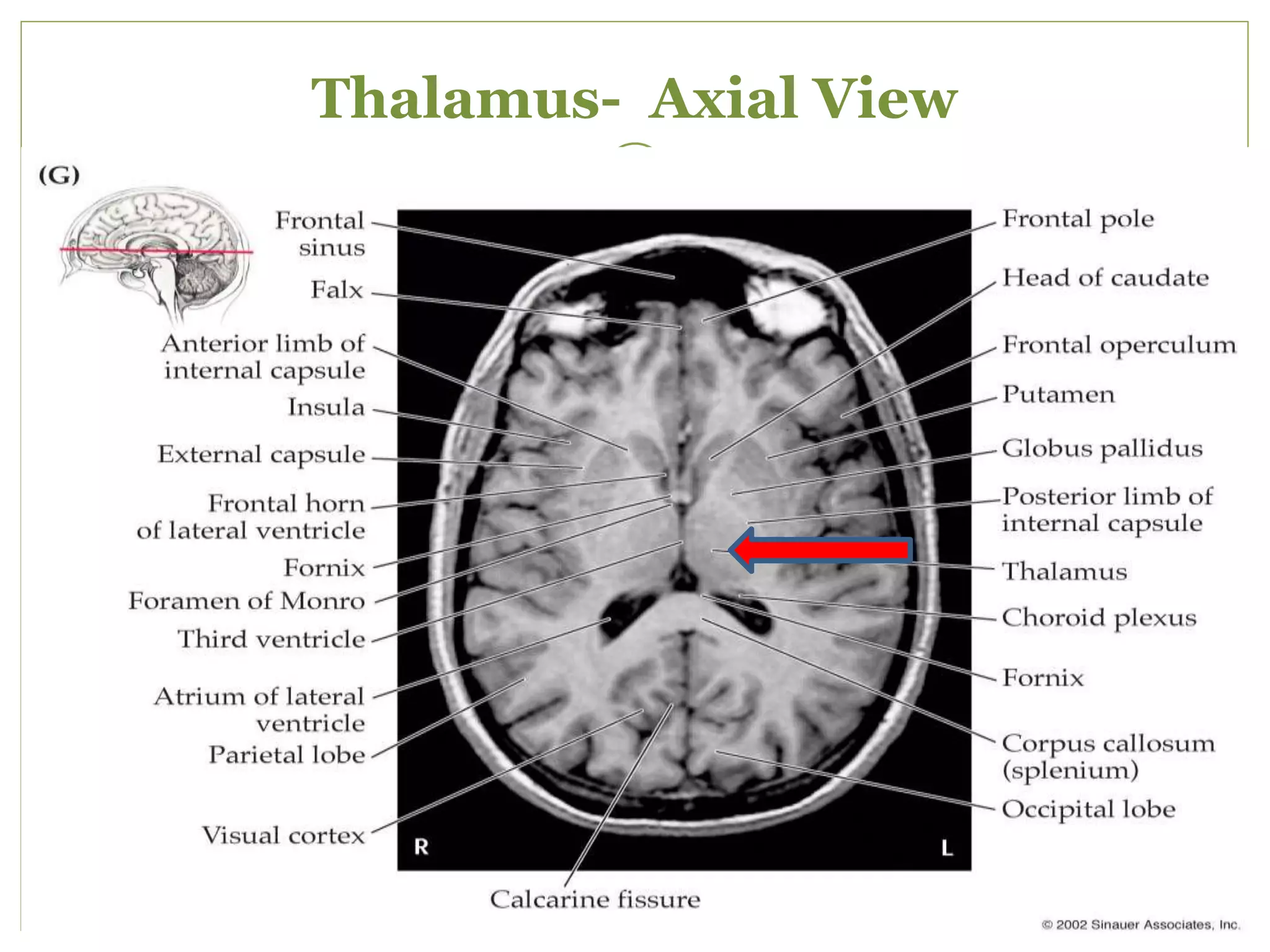
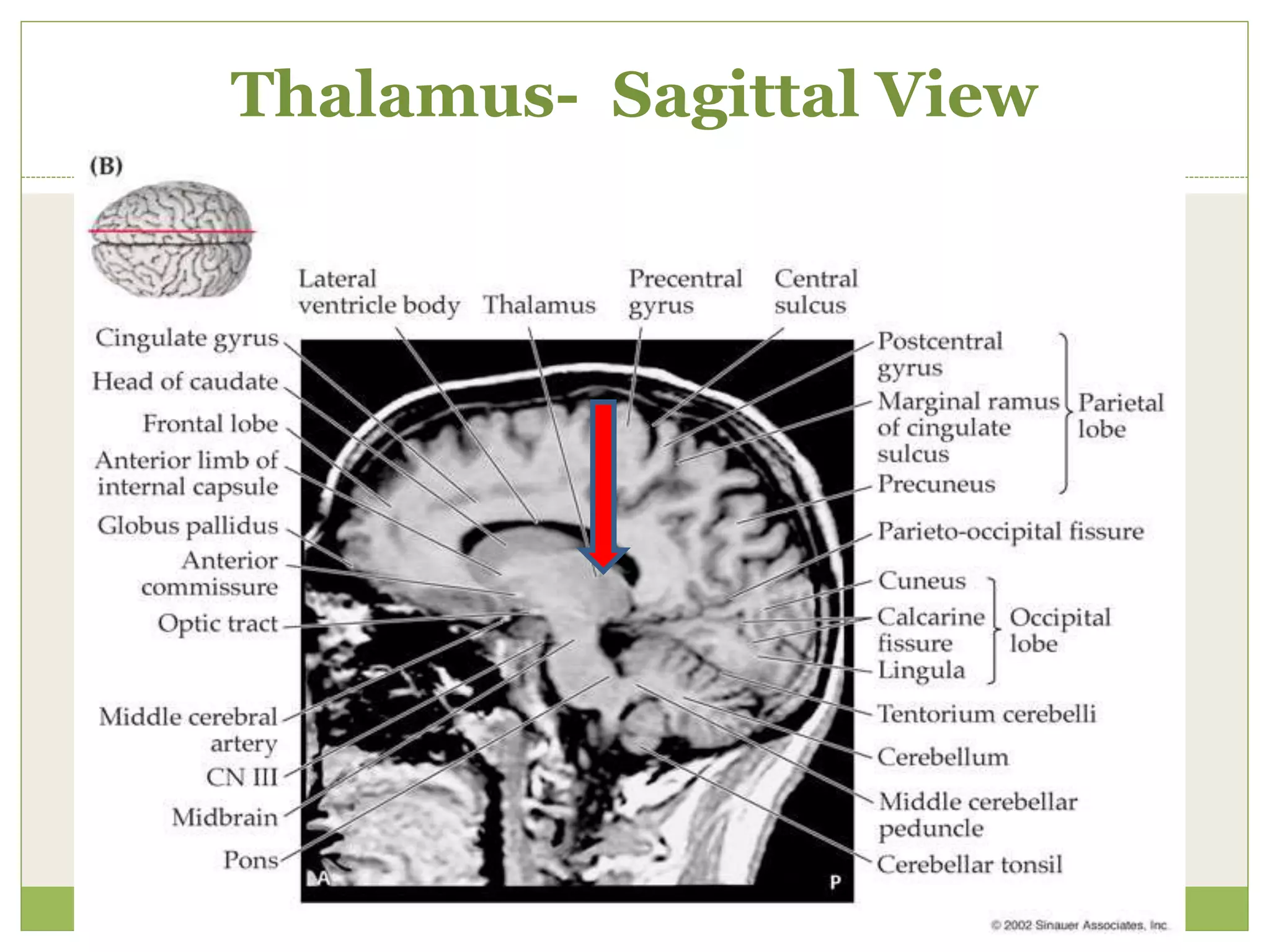


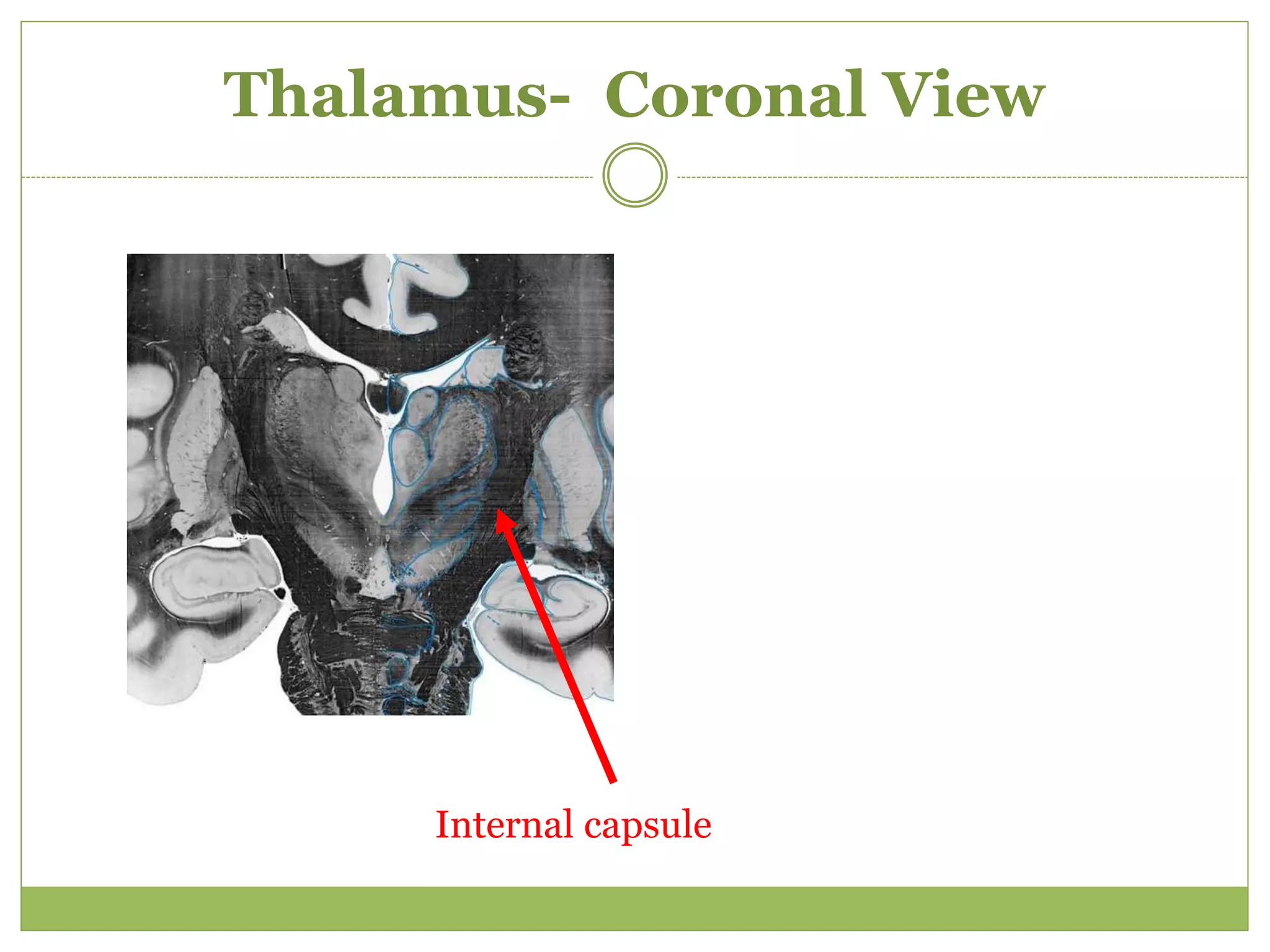


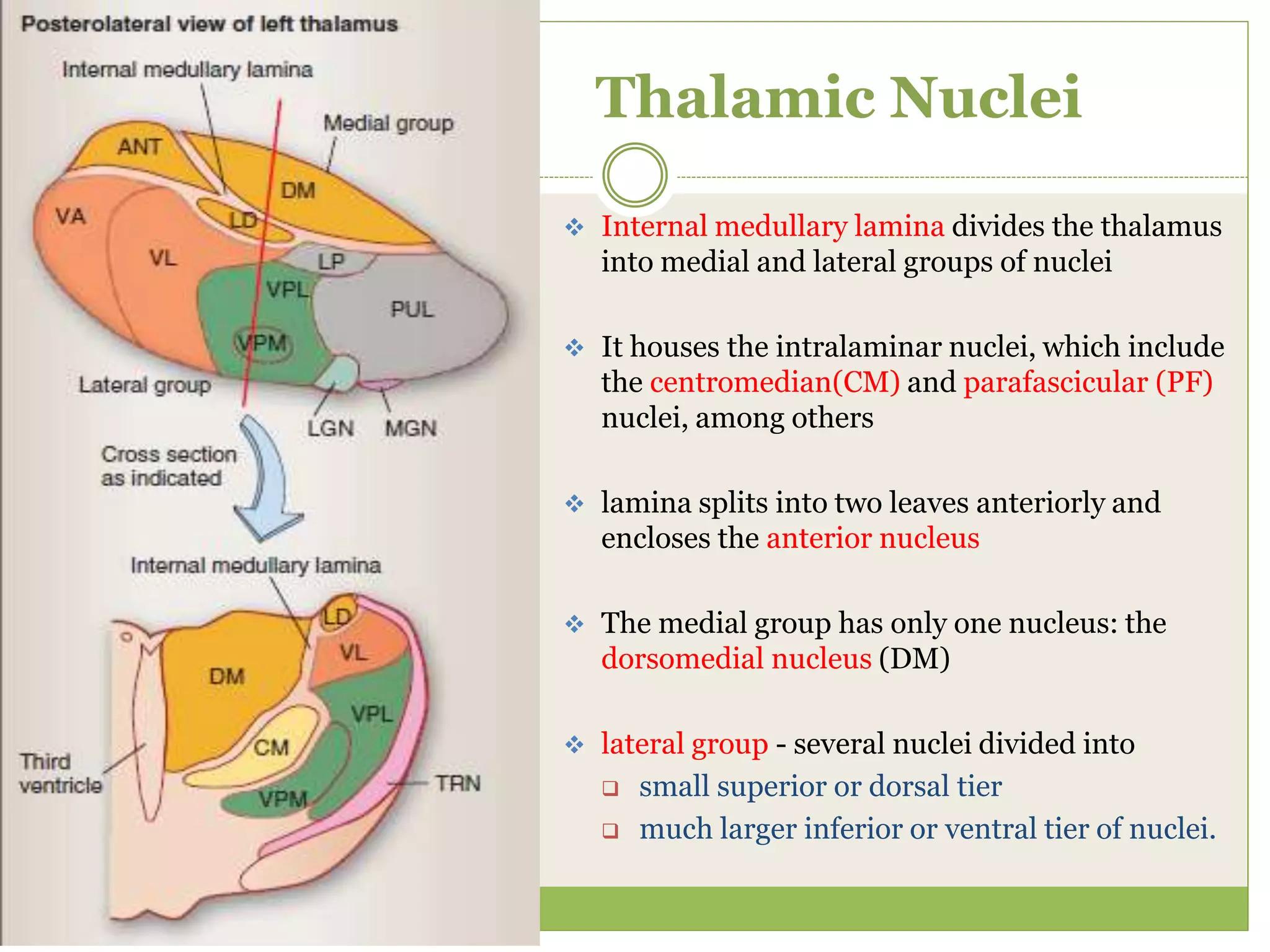































The thalamus is a paired symmetrical structure located in the center of the brain that relays sensory and motor signals between the brainstem and cerebral cortex. It is divided into several nuclei that have distinct connections and functions. The document provides detailed information on the anatomy, physiology, functional organization and clinical syndromes associated with lesions of different thalamic nuclei. Key points include a description of the gross anatomy and location of the thalamus, its blood supply, the nuclei and their connections, and syndromes associated with infarcts in the posterolateral and medial thalamic territories.



























































![080 - Neurology Physiology] Thalamus Anatomy & Function.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/080-neurologyphysiologythalamusanatomyfunction-241127085853-17b20927-thumbnail.jpg?width=640&height=640&fit=bounds)















































