Downloaded 284 times








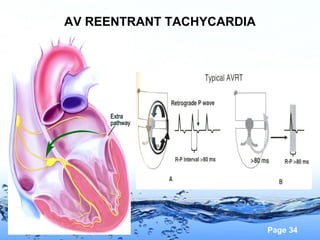
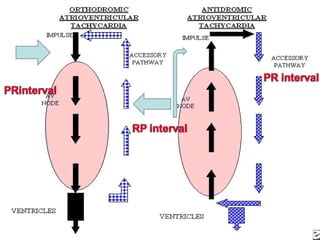
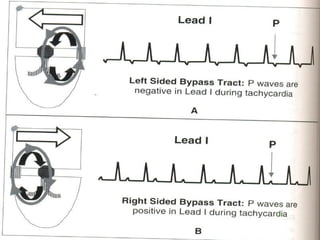
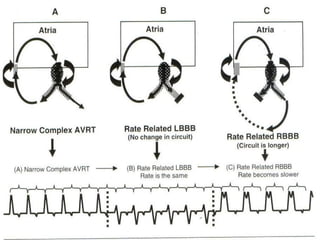



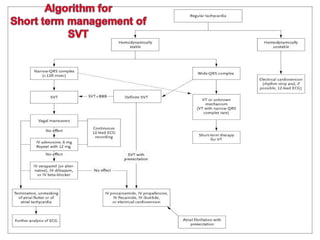
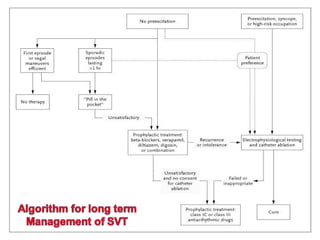
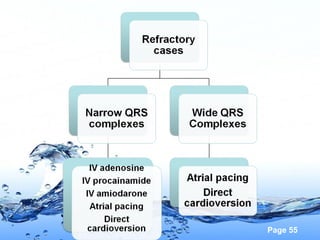









This document summarizes different types of cardiac arrhythmias including tachyarrhythmias and ventricular tachycardia. It discusses the mechanisms, classifications, diagnoses and treatments of supraventricular tachycardia including atrial flutter, atrial fibrillation, AV nodal reentrant tachycardia and AV reentrant tachycardia. It also covers ventricular tachycardia mechanisms including triggered activity, enhanced automaticity and reentry. Management strategies for acute and long term treatment of these arrhythmias are provided including electrical cardioversion, antiarrhythmic drug therapy and catheter ablation procedures.







































![Shadechapter14.ppt [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/shadechapter14-150421104301-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)
























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)










