1. Supraventricular tachycardia (SVT) refers to a group of tachyarrhythmias originating above the ventricles. Paroxysmal SVT is characterized by episodes of tachycardia with abrupt onset and termination.
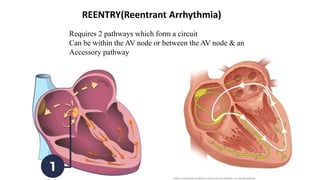
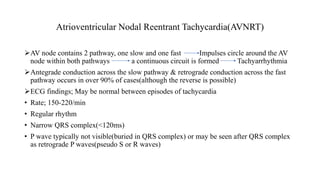
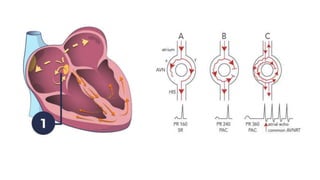
2. The main types of PSVT are atrioventricular nodal reentrant tachycardia (AVNRT), atrioventricular reentrant tachycardia (AVRT), and focal atrial tachycardia. They have different mechanisms and ECG patterns that can help determine the underlying rhythm.
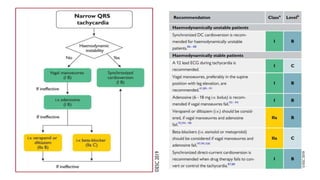
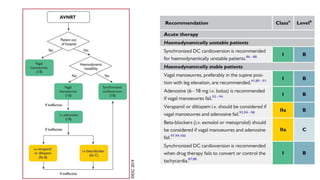
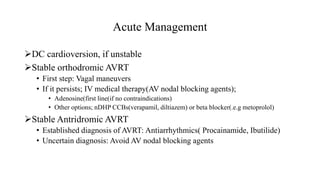
3. Acute management involves vagal maneuvers, medications like adenosine or beta blockers, or cardio






![An irregular SVT featuring ≥ 3 morphologies of P waves due to
multifocal origins of pacemaker activity
Etiology
• Severe underlying conditions (e.g., heart failure and pulmonary
diseases, such as COPD or pneumonia)
• Drugs (e.g., theophylline, isoproterenol) [52]
• Electrolyte abnormalities (e.g., hypokalemia, hypomagnesemia)
• Others: hypoxia, hypercapnia, acidosis](https://image.slidesharecdn.com/supraventriculartachycardia-231011203412-ed4dd47b/85/SupraventricularTachycardia-pptx-55-320.jpg)





















![Approach to palpitation [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/approachtopalpitationautosaved-170805225202-thumbnail.jpg?width=640&height=640&fit=bounds)






















































