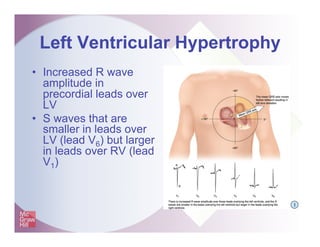
- Hypertrophy is a thickening of the ventricular wall, while dilation is an enlargement of a chamber to accommodate increased blood volume. Enlargement affects the atria, while hypertrophy affects the ventricles.
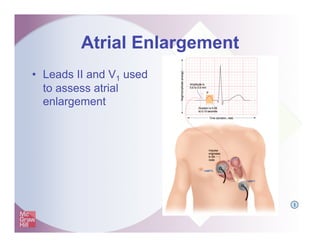
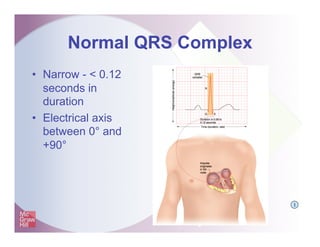
- The P wave is used to identify atrial enlargement, while changes in the QRS complex indicate ventricular hypertrophy. Increased duration, amplitude or axis deviation serve as indicators.
- Right atrial enlargement increases the first part of the P wave amplitude. Left atrial enlargement increases the terminal P wave amplitude in V1 and the P wave duration.
























![Shadechapter13.ppt [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/shadechapter13-150421104054-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Shadechapter12.ppt [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/shadechapter12-150421103821-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Shadechapter15.ppt [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/shadechapter15-150421104606-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Shadechapter09.ppt [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/shadechapter09-150421103043-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Shadechapter11.ppt [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/shadechapter11-150421103622-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Shadechapter05.ppt [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/shadechapter05-150421102328-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Shadechapter16.ppt [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/shadechapter16-150421104734-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Shadechapter10.ppt [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/shadechapter10-150421103304-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Shadechapter07.ppt [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/shadechapter07-150421102520-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Shadechapter01.ppt [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/shadechapter01-150421101218-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Shadechapter02.ppt [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/shadechapter02-150421101545-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)








![ECG & Heart block [doctors online]](https://cdn.slidesharecdn.com/ss_thumbnails/ecgheartblockdoctorsonline-131111054313-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)

![Shadechapter08.ppt [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/shadechapter08-150421102734-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)

































































