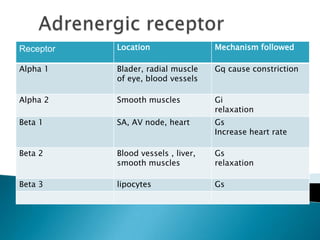
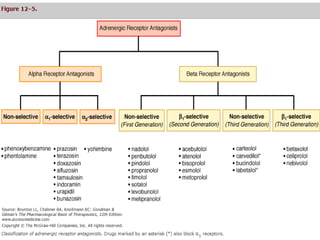


Adrenergic blocking agents, also known as adrenergic antagonists, block alpha and/or beta receptor sites and have the opposite effect of adrenergic agents. They are classified based on the type of adrenergic receptor they block, including alpha1, alpha2, beta1, beta2, and beta3 receptors. Common uses include treatment of hypertension, heart failure, and benign prostatic hyperplasia. Side effects may include hypotension, tachycardia, and bronchospasm.





































































































