Downloaded 61 times


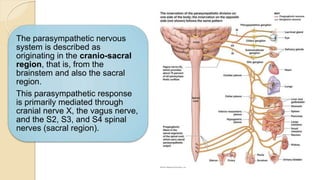

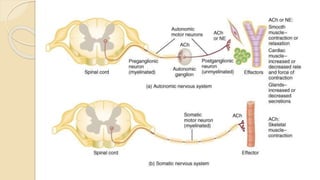
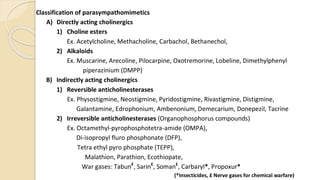
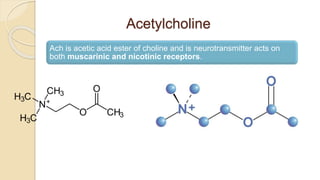

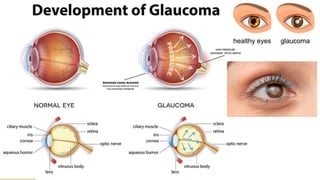
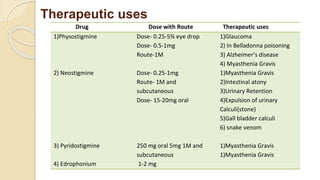



The document discusses the parasympathetic nervous system and parasympathomimetic drugs. It provides details on: - The parasympathetic nervous system originates from the brainstem and sacral region and uses acetylcholine as a neurotransmitter. - Parasympathomimetic drugs like acetylcholine, muscarine, and anticholinesterases act to stimulate parasympathetic responses. Direct acting drugs activate cholinergic receptors while indirect drugs inhibit acetylcholinesterase. - These drugs have therapeutic uses for conditions like glaucoma, urinary retention, and myasthenia gravis. Combinations of drugs are sometimes used to achieve optimal effects while minimizing side effects.





















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)

