Downloaded 98 times

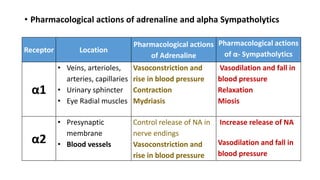






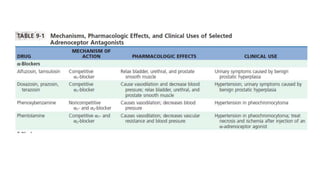













The document provides an overview of sympatholytic drugs, specifically focusing on alpha and beta adrenergic blockers that inhibit the effects of adrenergic neurotransmitters. It details the pharmacological actions, therapeutic uses, and adverse effects of alpha sympatholytics in managing conditions like hypertension and pheochromocytoma, as well as the mechanisms and uses of beta blockers in various cardiac and non-cardiac conditions. The document also includes the adrenaline reversal phenomenon and discusses classifications of sympatholytics.























































































