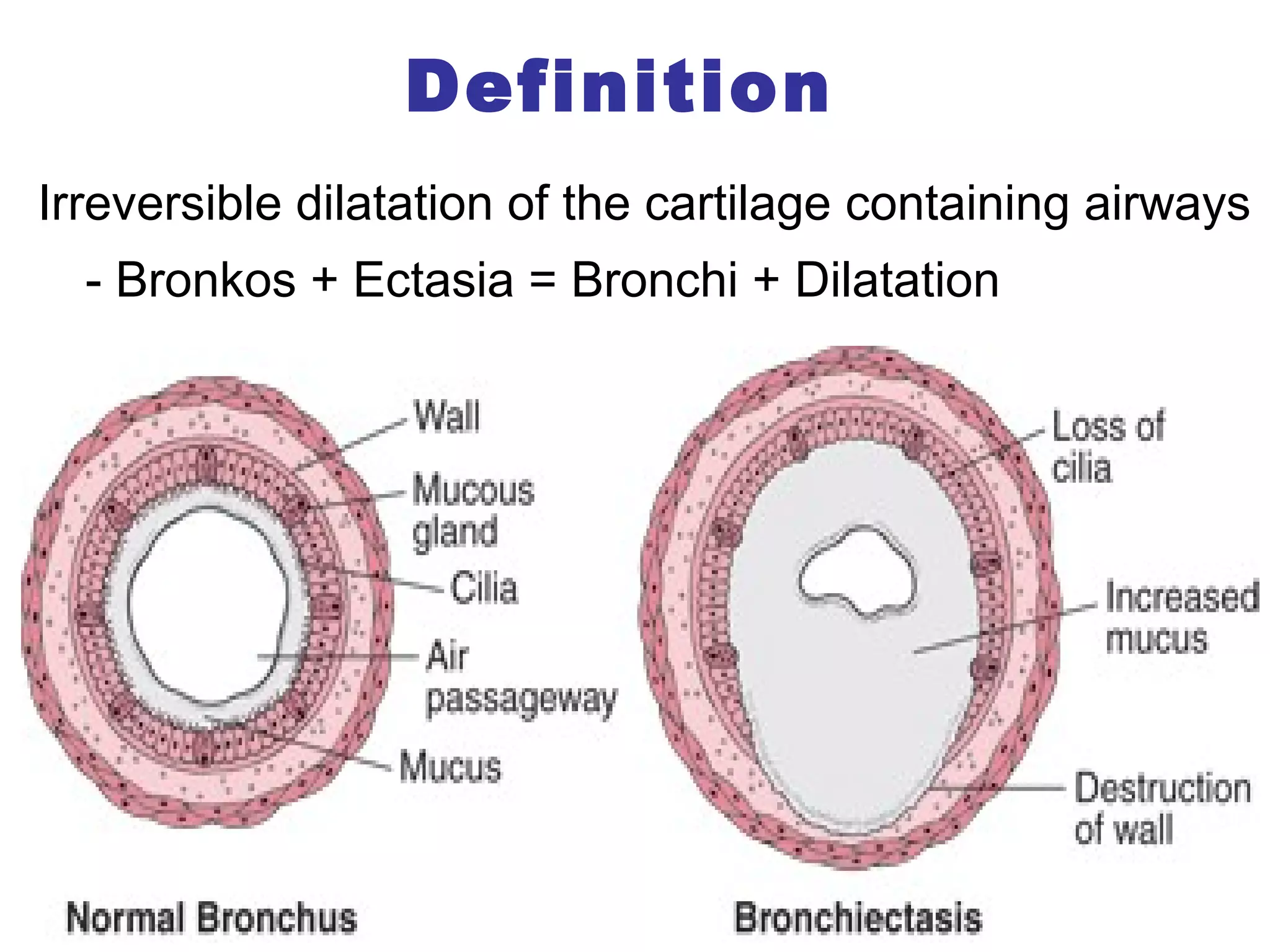






















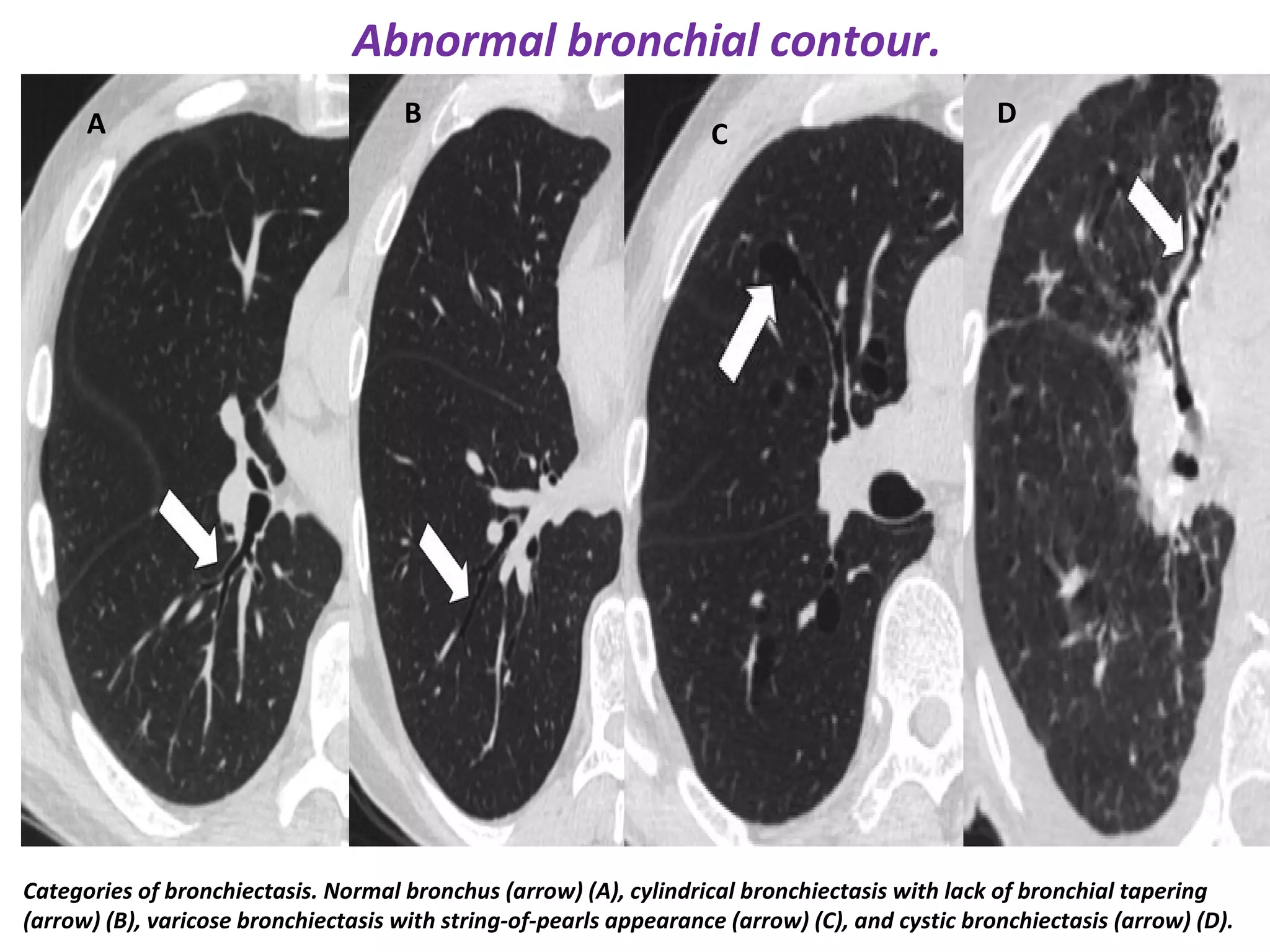


































This document discusses suppurative lung diseases including bronchiectasis, lung abscesses, and empyema with broncho-pleural fistula. It defines the conditions, describes causes, clinical features, investigations, and treatment approaches. Key points include that bronchiectasis is irreversible dilatation of airways leading to infection and damage, lung abscesses begin as areas of pneumonia that progress to cavitation, and empyema is pus in the pleural space that can form a fistula with the bronchial tree through various causes like pneumonia or lung abscess rupture. Treatment involves controlling infections, clearing secretions, and surgery in chronic or complicated cases.








































































































