Downloaded 42 times

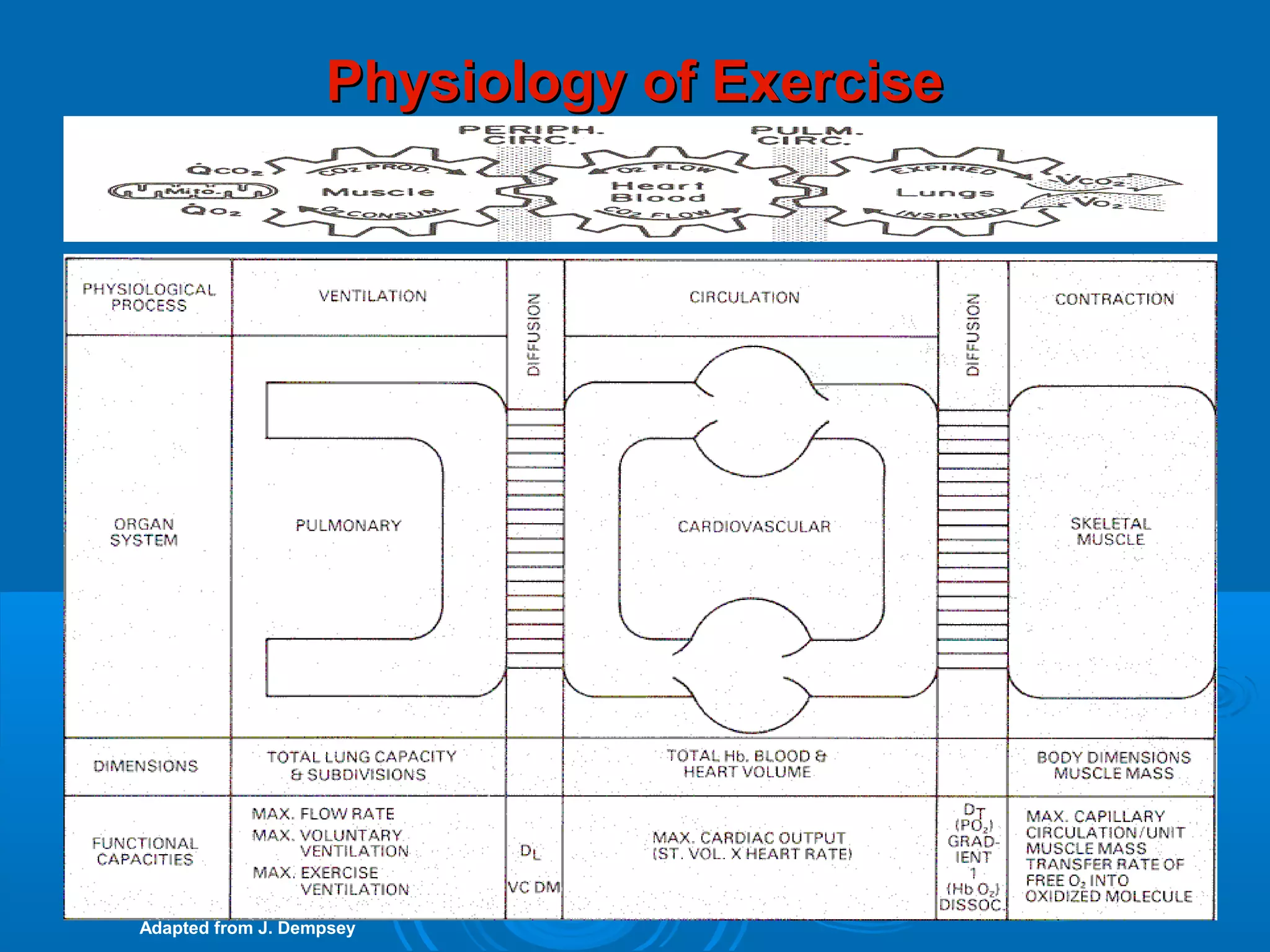
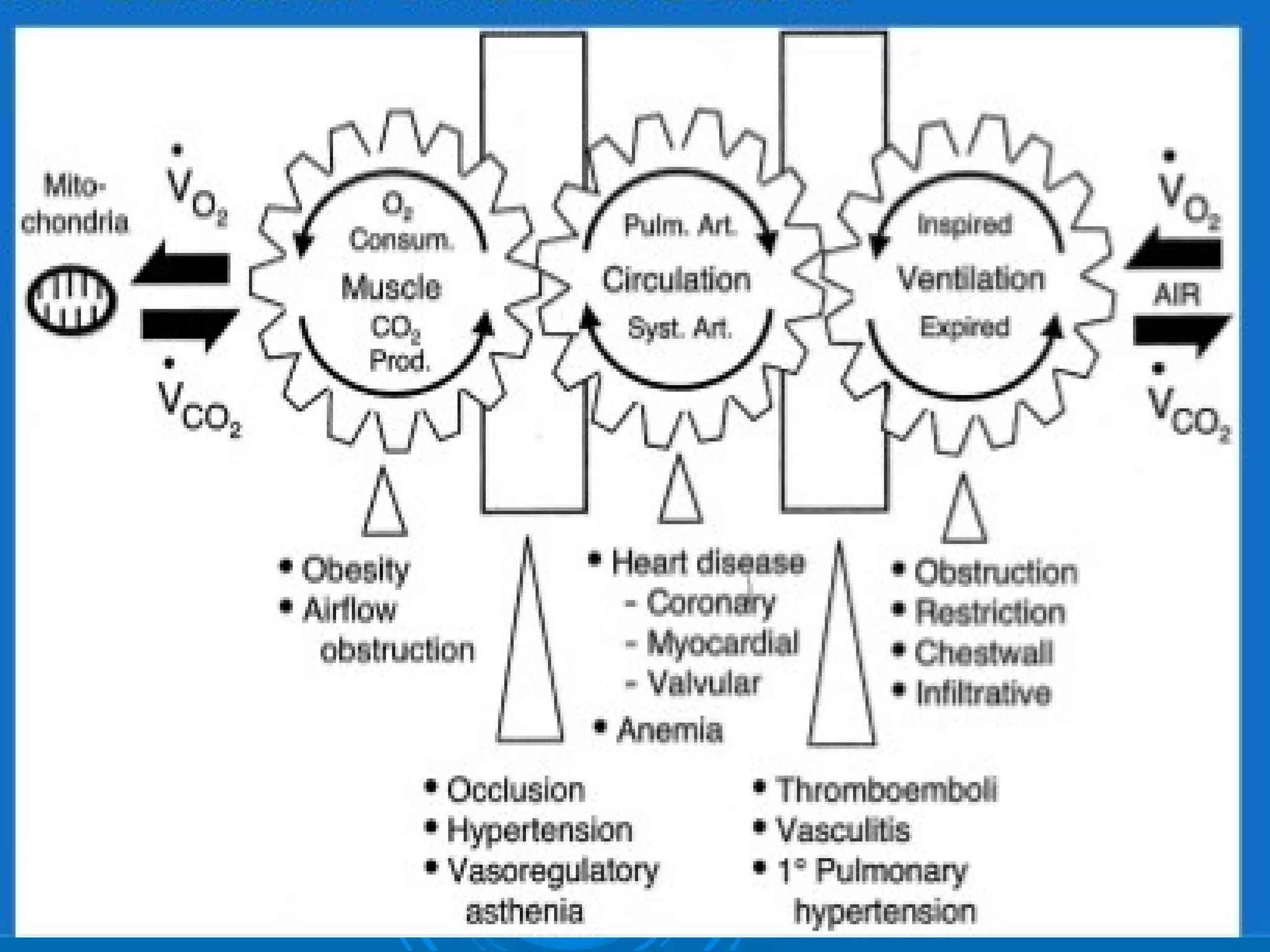

















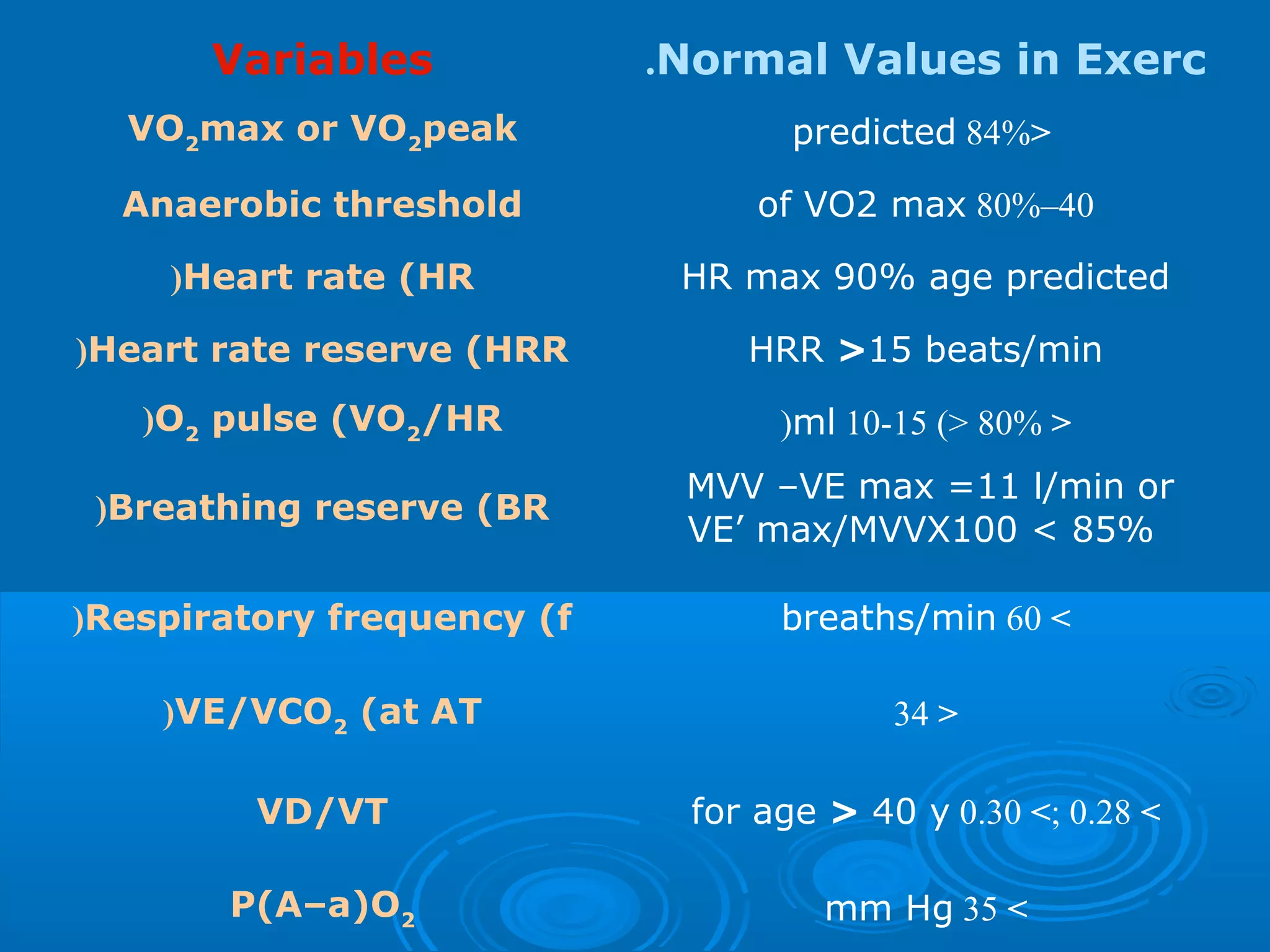



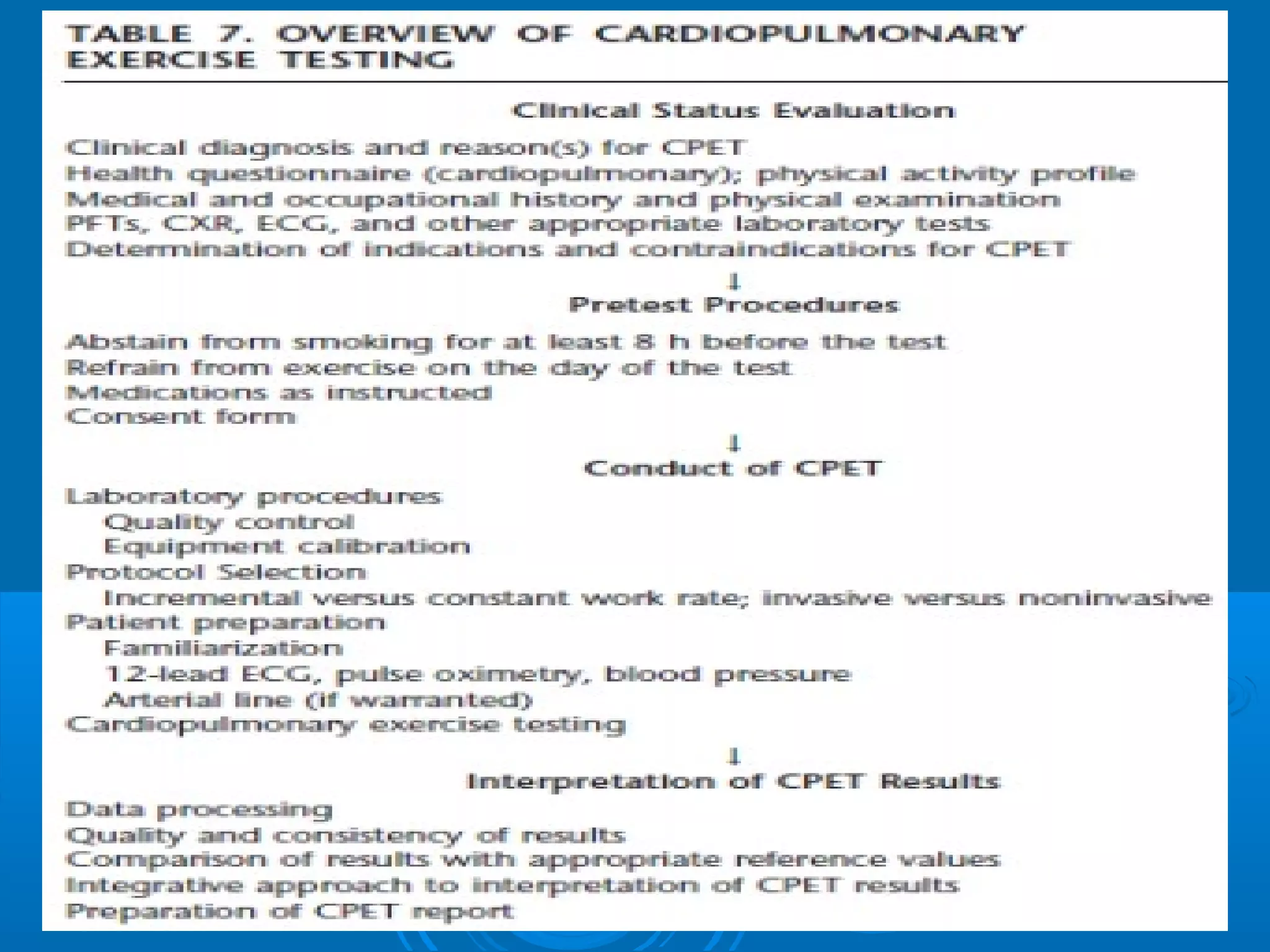



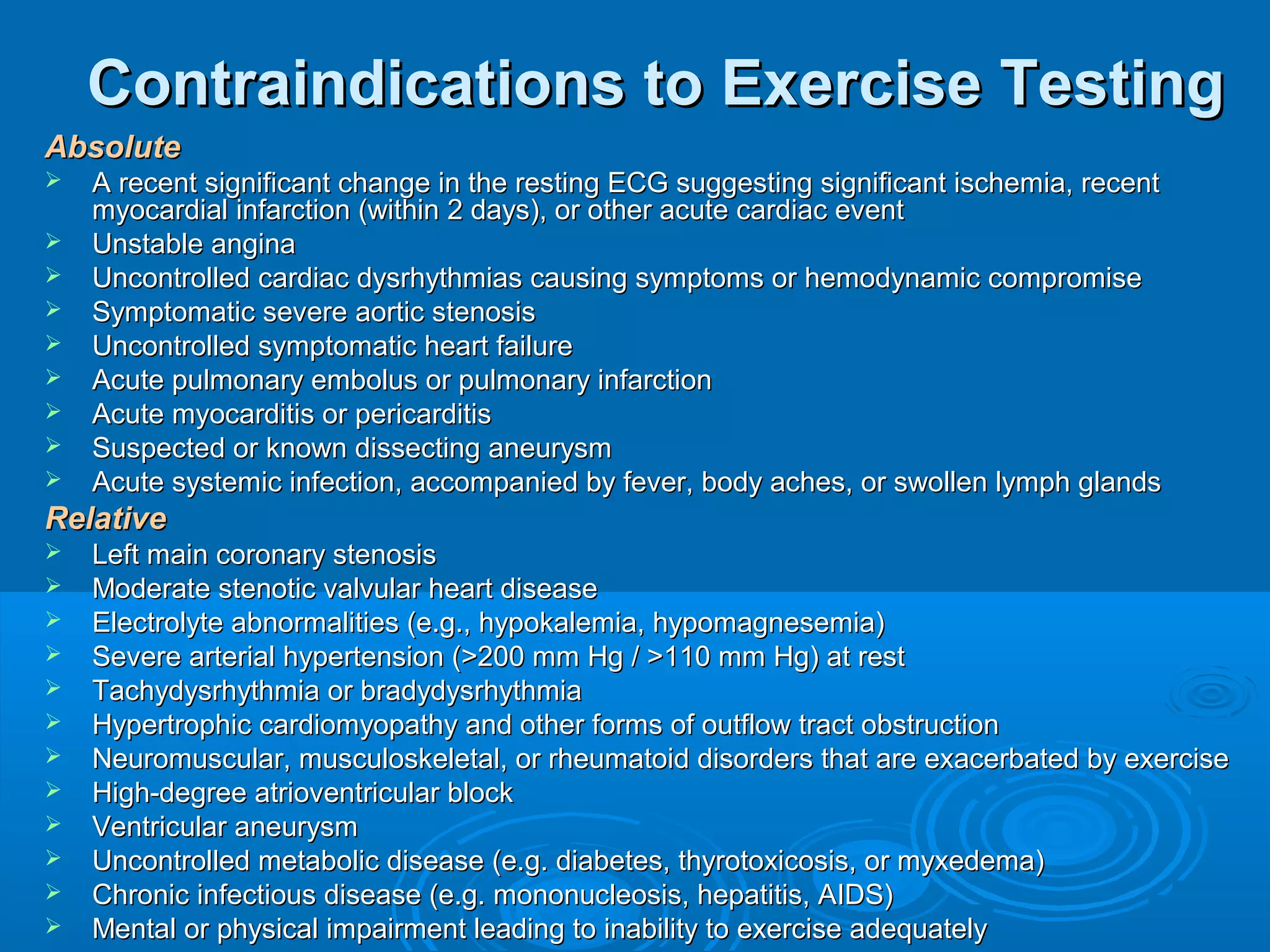








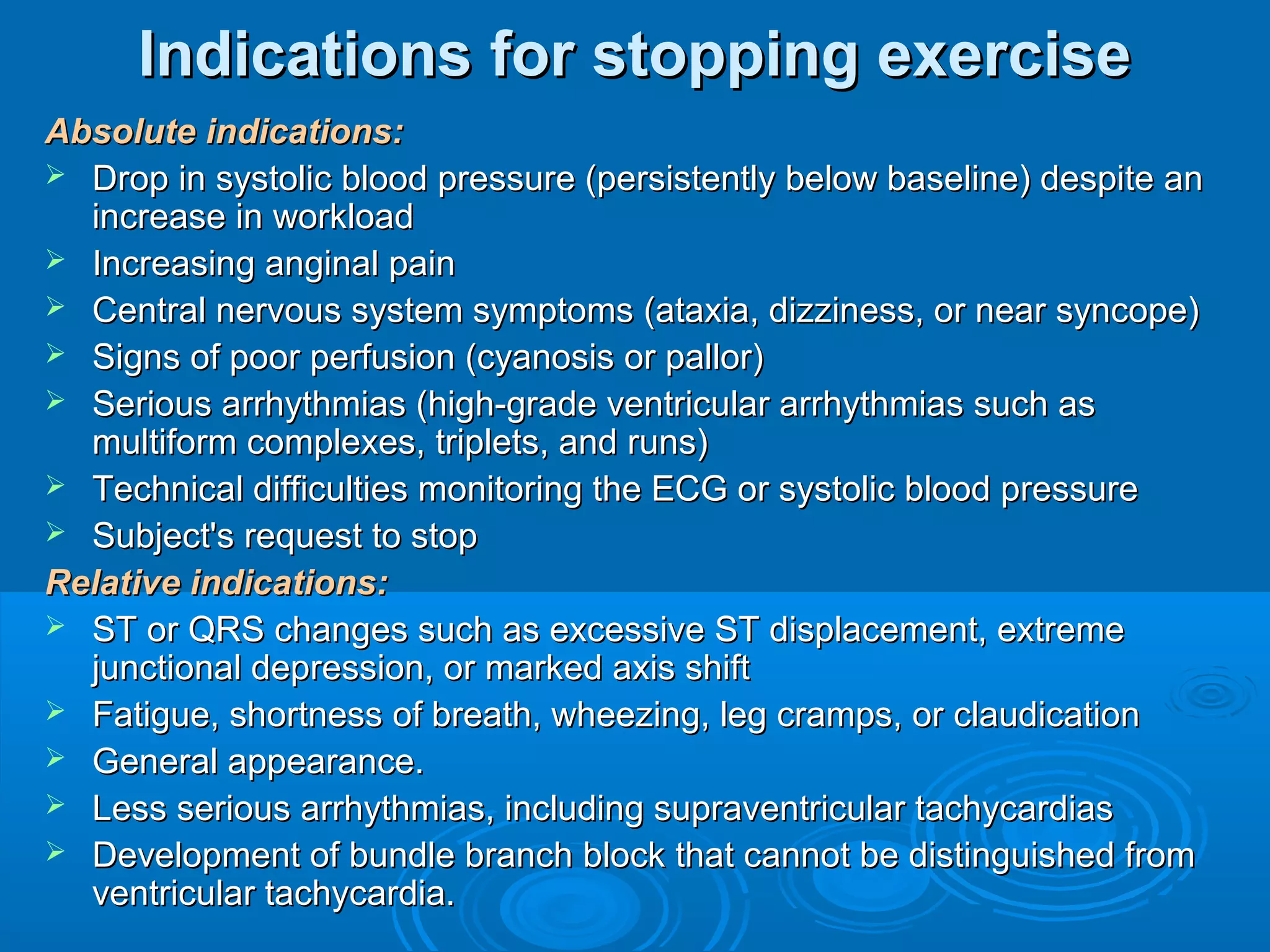







- The document discusses the physiology of exercise and cardio-pulmonary exercise testing. It describes the process of external and internal respiration during exercise. Key metabolic parameters discussed include oxygen consumption, carbon dioxide production, anaerobic threshold, and respiratory quotient. Pulmonary parameters examined include minute ventilation, tidal volume, respiratory rate, and alveolar-arterial oxygen difference. Cardiovascular parameters outlined are cardiac output, stroke volume, and heart rate.























































































