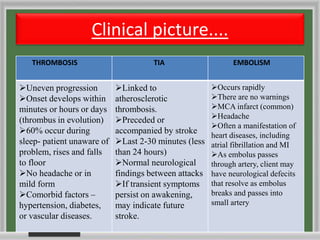
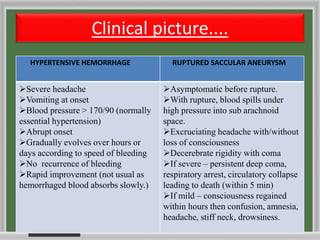
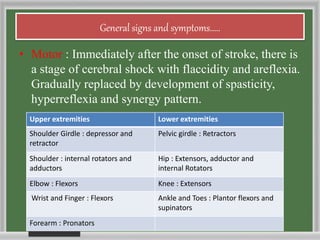
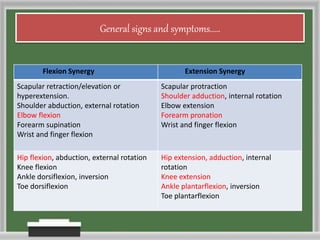
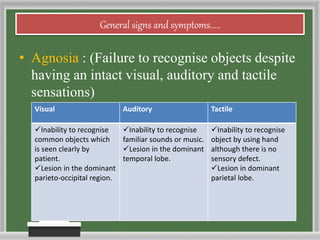
The document summarizes the clinical manifestations of strokes. It describes the differences between thrombotic, embolic, and hemorrhagic strokes and how their symptoms vary based on the location and size of the brain lesion. It then provides details on specific types of strokes like TIAs, thromboses, embolisms, and aneurysms. Finally, it outlines the general signs and symptoms that can result from strokes like sensory and motor deficits, reflex changes, apraxia, aphasia, and cognitive impairments.