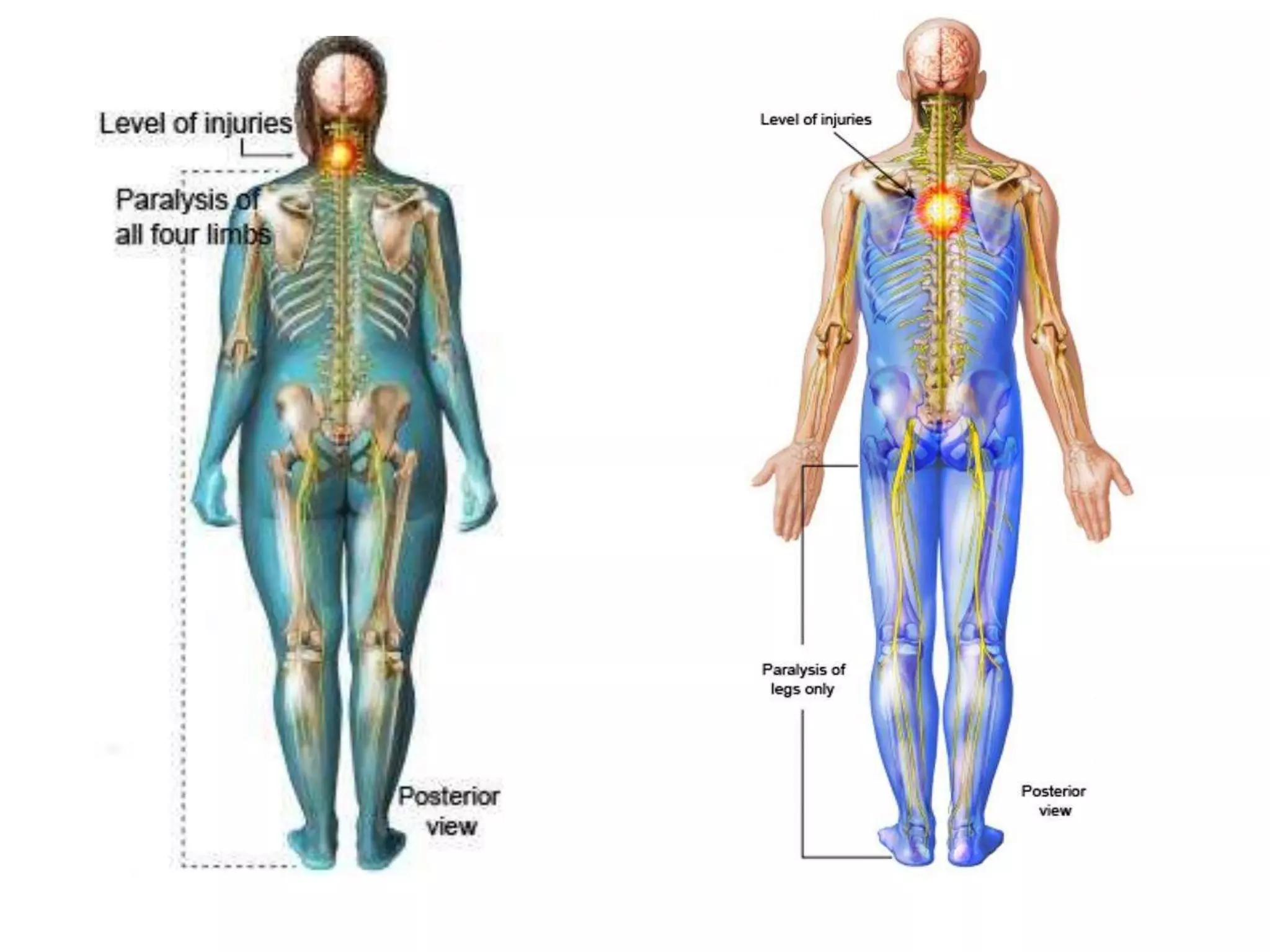
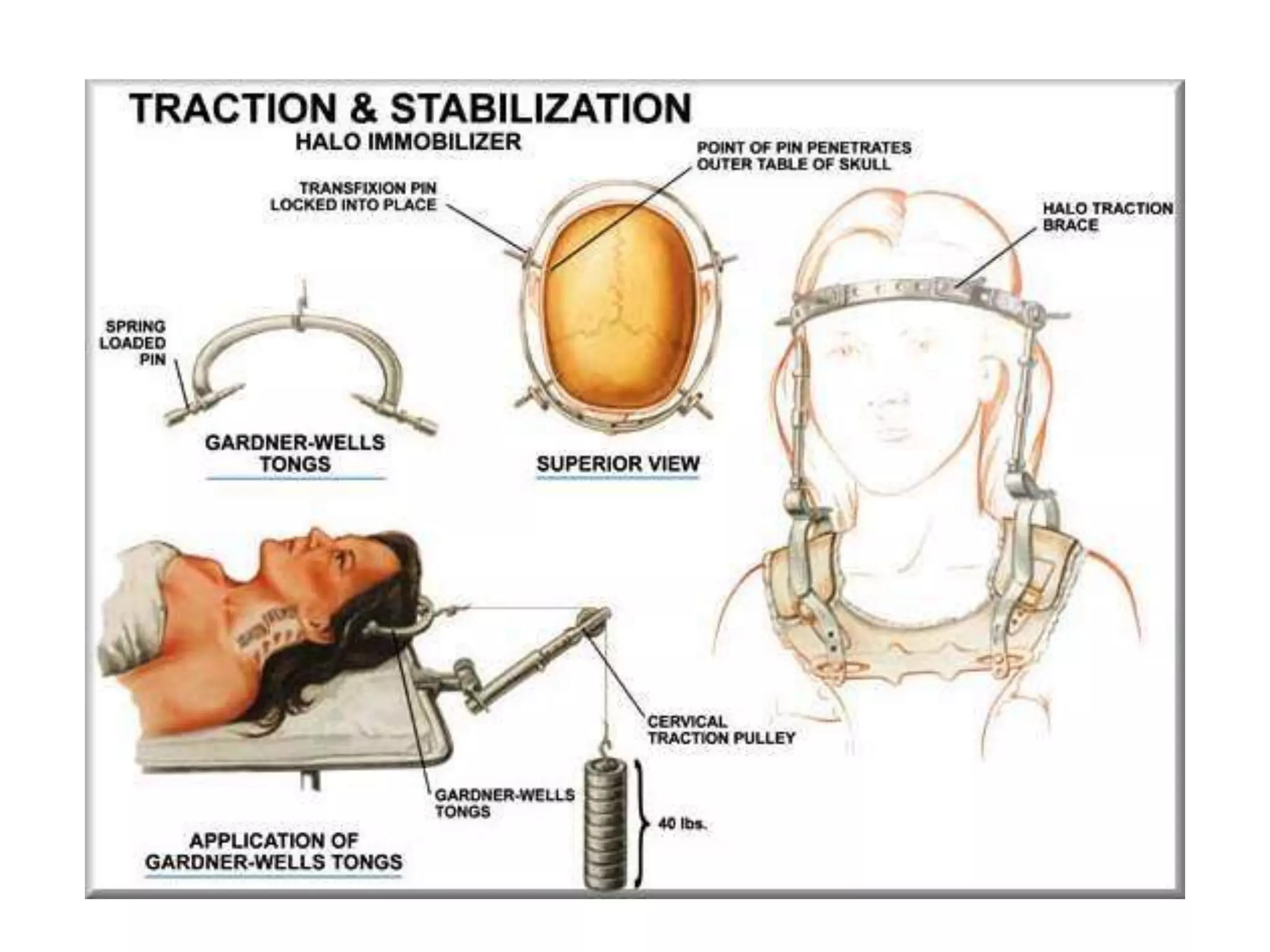
Quadriplegia is paralysis of both arms and legs caused by injury to the cervical spinal cord. Paraplegia is paralysis of the lower half of the body caused by injury to the thoracic, lumbar, or sacral spinal cord. Management of spinal cord injuries involves immobilization, medications like methylprednisolone, and surgery to stabilize the spine. Physical therapy focuses on range of motion, strengthening, pain management, and retraining bladder and bowel function to prevent complications like pressure sores. Functional electrical stimulation has also been used to facilitate walking.