
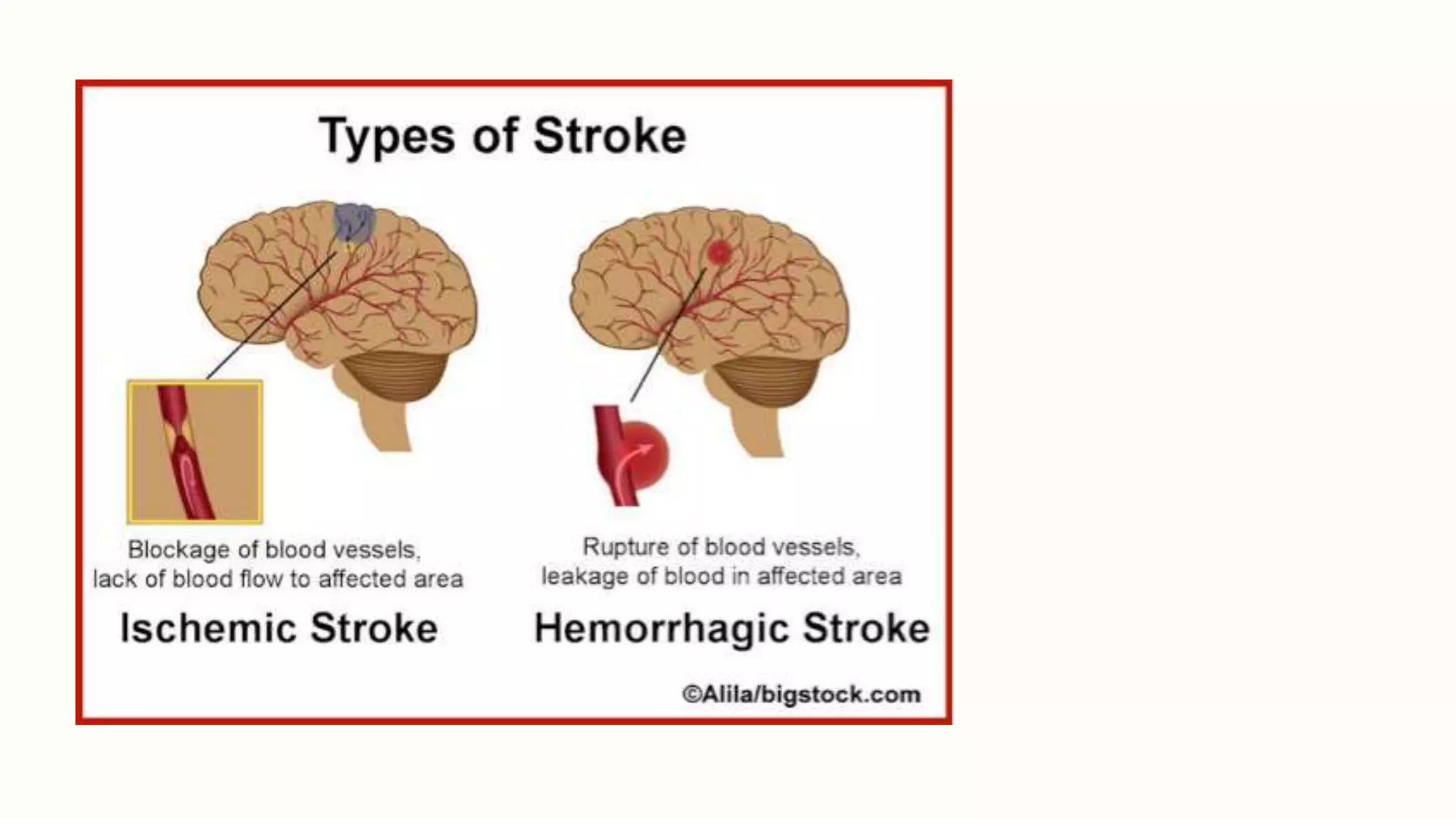

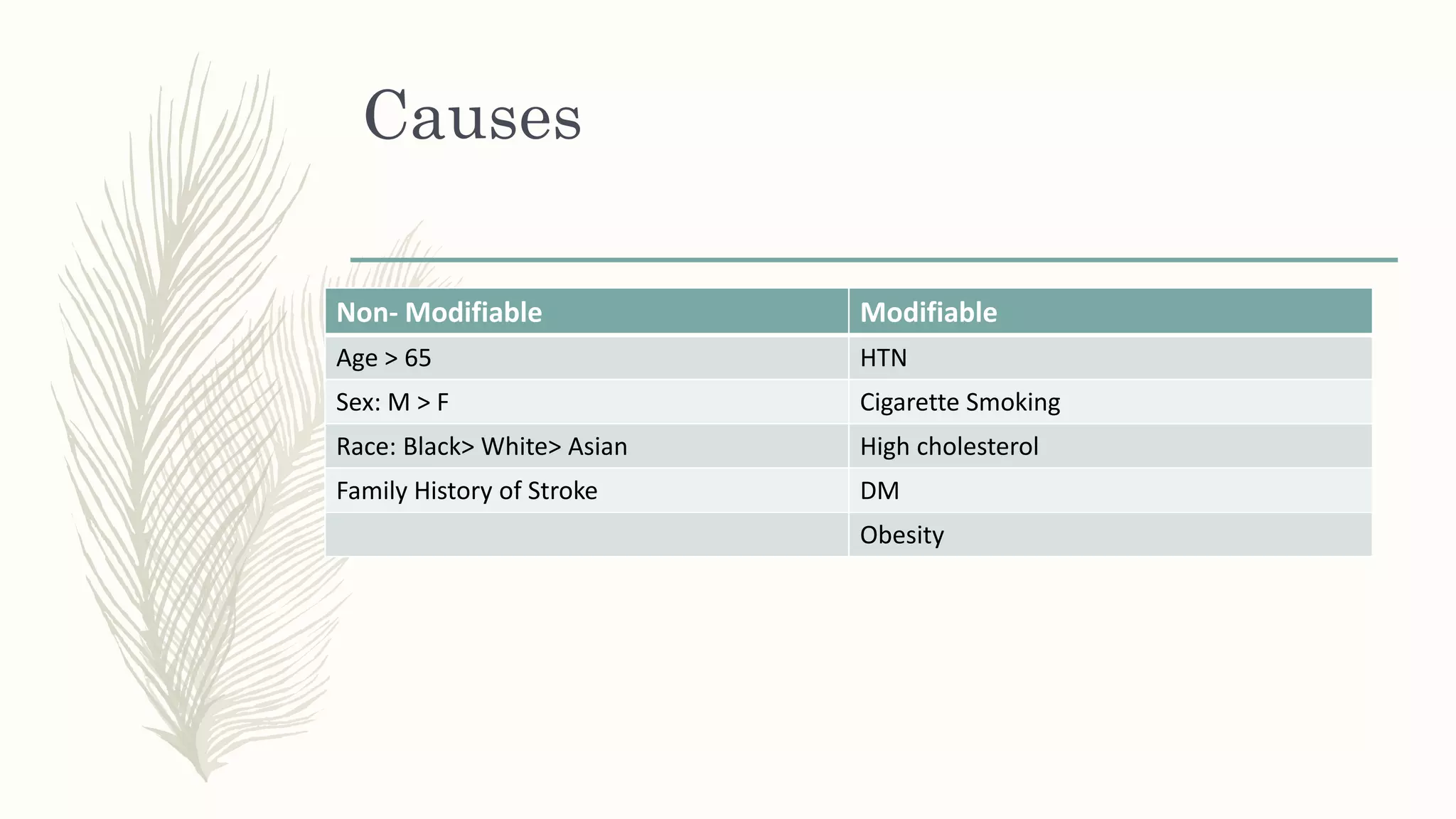






The document presents a comprehensive overview of ischaemic stroke, covering its anatomy, definition, causes, pathophysiology, and management strategies including acute and surgical interventions. It includes case studies detailing patient demographics, symptoms, diagnosis, and physical therapy management while emphasizing the importance of rapid assessment and treatment for optimal recovery outcomes. Additionally, it highlights epidemiological data and the implications of common complications associated with stroke.




























































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)













