Download as PDF, PPTX














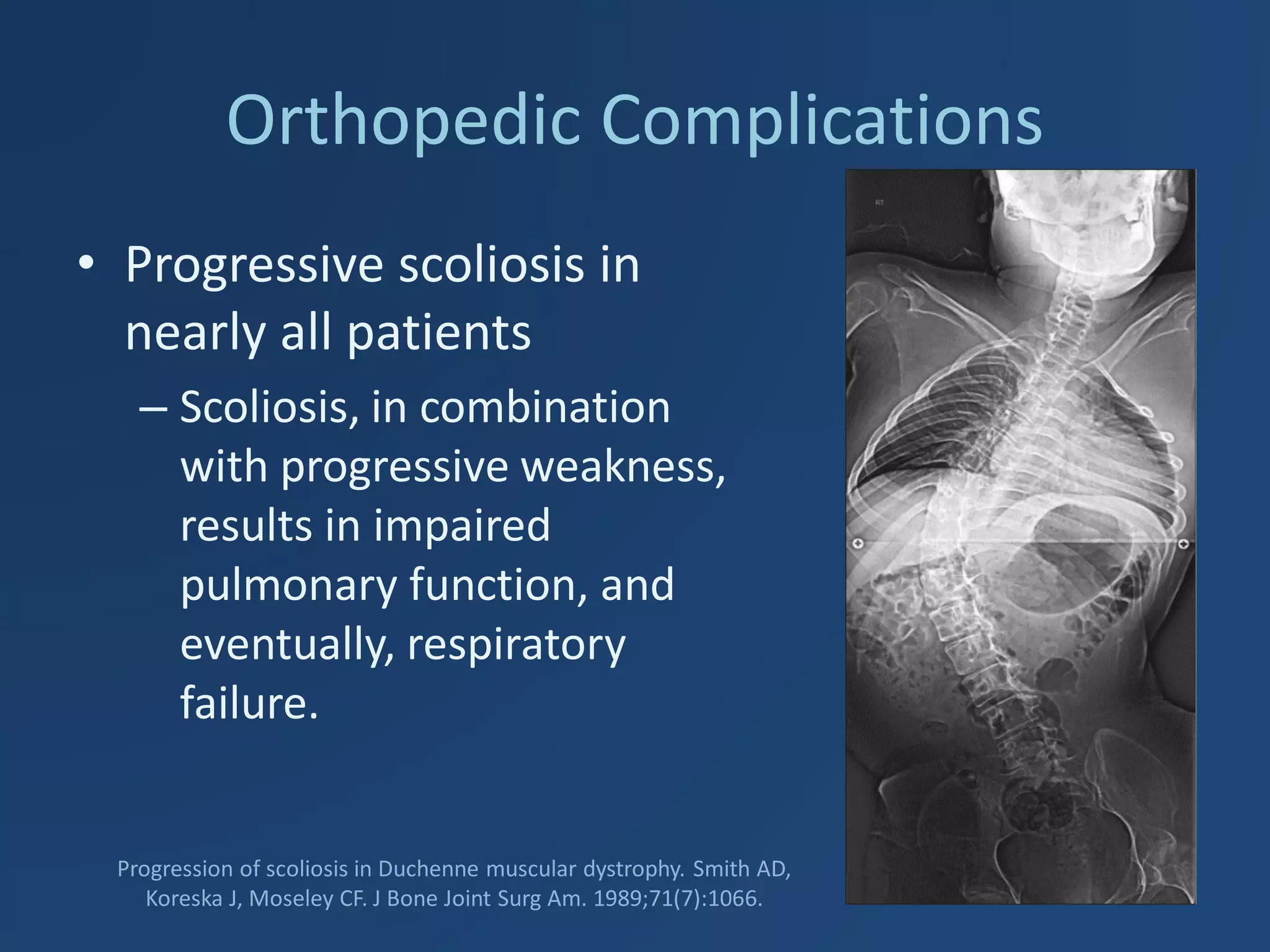

















Duchenne Muscular Dystrophy (DMD) is a genetic disorder caused by mutations in the dystrophin gene leading to progressive muscle weakness. It mainly affects boys and symptoms start between ages 2-3. Affected children become wheelchair bound by age 12 and have life-threatening heart, respiratory, and orthopedic complications if not properly managed. Management involves monitoring for cardiomyopathy, respiratory support, orthopedic care, corticosteroids which can prolong ambulation, and future therapies like gene therapy aim to treat the underlying genetic cause.









































































