Downloaded 886 times

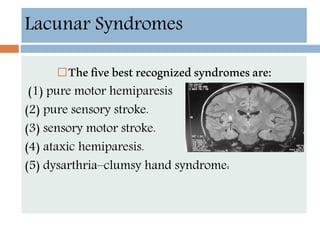
![Neuroprotection
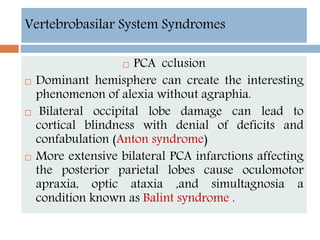
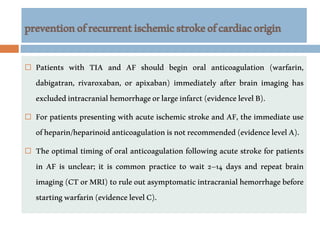
Currently, data are inadequate to justify the
routine use of heparin or other anticoagulants in
the acute management of ischemic stroke.[126]
Patients with embolic stroke who have another
indication for anticoagulation (eg, atrial
fibrillation) may be placed on anticoagulation
therapy nonemergently, with the goal of
preventing further embolic disease; however, the
potential benefits of that intervention must be
weighed against the risk of hemorrhagic
transformation.[1] For more information](https://image.slidesharecdn.com/ischaemicstrokeppt-160812010715/85/Ischaemic-stroke-55-320.jpg)


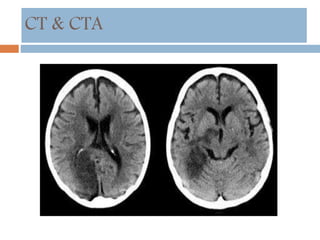
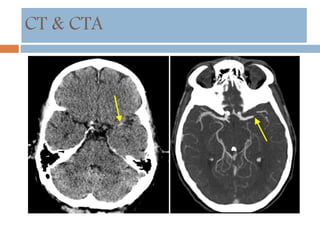
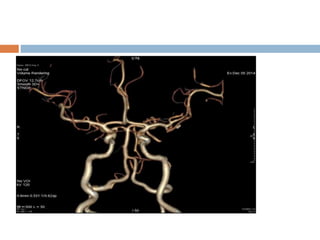
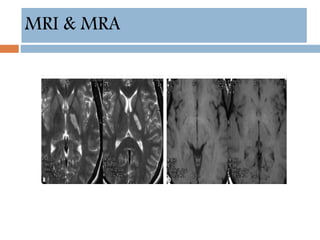
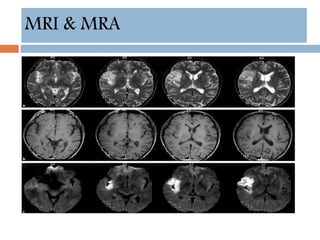
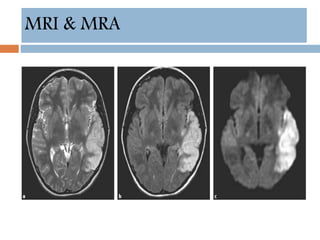
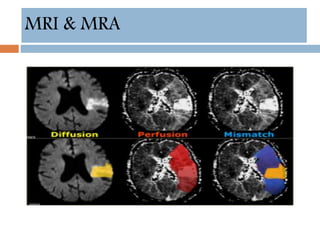
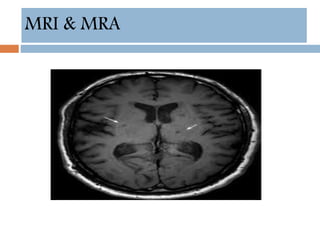
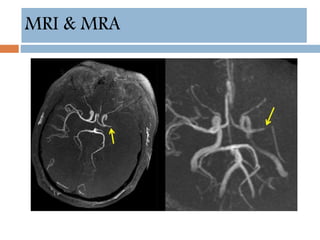
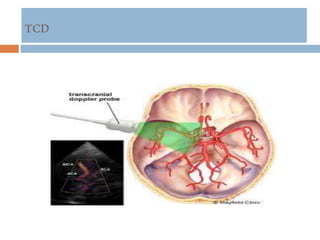
This document provides an overview of ischaemic stroke, including its definition, risk factors, pathophysiology, clinical presentation, diagnosis and management. Key points include: - Ischaemic stroke accounts for 80% of strokes and results from focal brain infarction due to obstruction of cerebral blood flow. - Major risk factors include hypertension, atrial fibrillation, diabetes, hyperlipidemia and previous stroke or TIA. - Clinical syndromes depend on the location of brain infarction and can include motor/sensory deficits, aphasia and visual field cuts. - Diagnosis involves neuroimaging such as CT, MRI and vascular imaging to identify the cause. - Acute



























































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)





![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)









