Downloaded 1,547 times












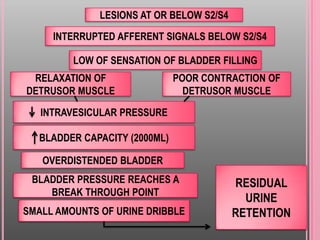


Neurogenic bladder refers to urinary bladder dysfunction caused by diseases of the central or peripheral nervous system that control urination. There are two main types: a flaccid bladder that does not contract fully, causing urine to dribble out continuously, and a spastic bladder with involuntary contractions causing frequent urination. Common causes include stroke, Parkinson's, MS, spinal cord injuries, and neurological disorders from conditions like diabetes. Symptoms include frequent urination, incontinence, and urinary retention. Treatment involves medications to relax or stimulate the bladder along with exercises and sometimes surgery.