The document discusses stroke, including its definition, causes, risk factors, symptoms, assessment, recovery stages, and complications. Key points include:
- Stroke is defined as sudden neurological dysfunction due to abnormal cerebral circulation lasting over 24 hours.
- Common causes include atherosclerosis, cerebral thrombus, embolism from the heart.
- Risk factors include hypertension, diabetes, heart disease, smoking, obesity.
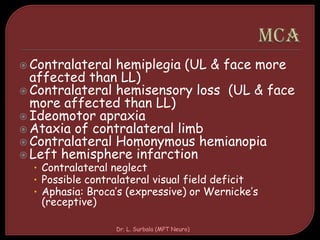
- Symptoms can include weakness, numbness, vision issues, speech problems.
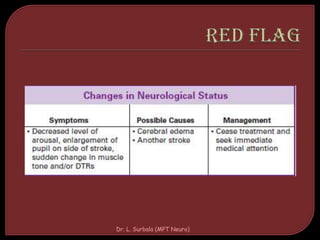
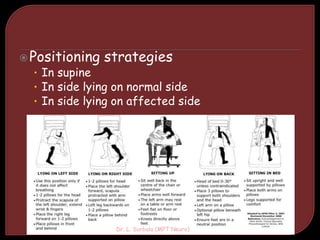
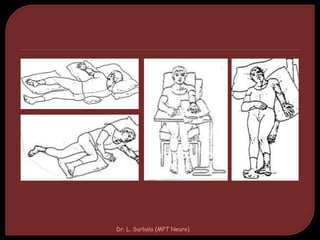
- Recovery is assessed based on severity, duration, and affected brain region. Complications can include contractures, seizures, DVT.