Downloaded 1,052 times
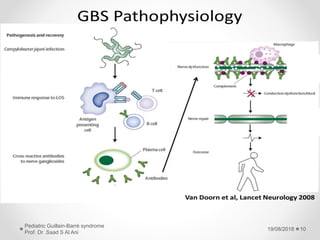
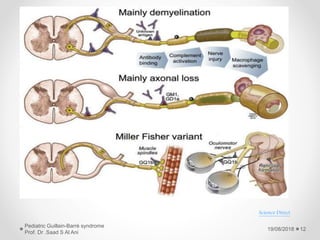
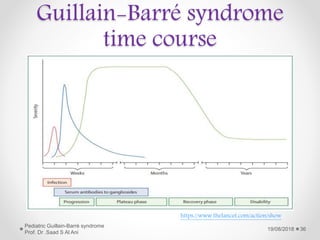



Guillain-Barré syndrome (GBS) is an acute inflammatory polyradiculoneuropathy that causes weakness and diminished reflexes. It is typically characterized by an acute monophasic illness manifesting as ascending weakness and areflexia following a gastrointestinal or respiratory infection. The classic presentation is acute inflammatory demyelinating polyradiculoneuropathy but it can also present as acute axonal forms that damage nerve axons. Diagnosis is based on progressive ascending weakness, areflexia, and supportive findings on lumbar puncture, electrodiagnostic studies, and occasionally MRI.























































































