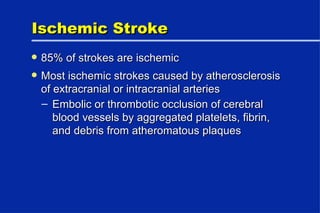
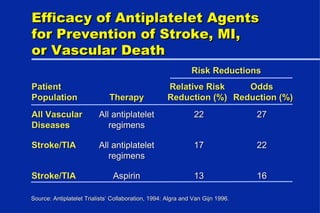
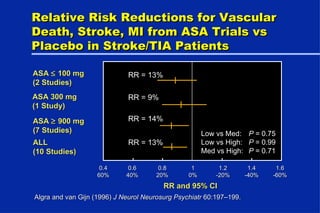
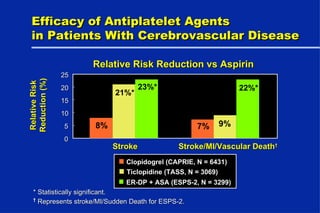
- The document discusses secondary prevention of ischemic stroke through the use of antiplatelet agents such as aspirin, ticlopidine, and clopidogrel. These antiplatelet agents provide a modest reduction in risk of non-fatal stroke and death.
- While antiplatelet therapy is effective, more effective and safe treatment options are still needed given the devastating consequences of stroke.
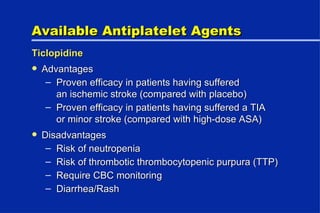
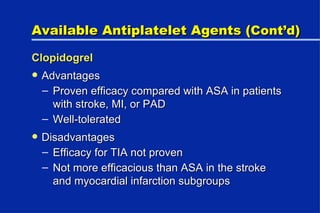
- Acceptable options for initial antiplatelet therapy include aspirin, clopidogrel, ticlopidine, and the combination of aspirin and dipyridamole. Clopidogrel is preferred over ticlopidine due to fewer side effects.




![FDA Recommends Low-Dose Aspirin FDA reviewed trials of aspirin vs placebo The “positive findings at lower dosages are sufficient reason to lower the dosage of aspirin...for subjects with TIA and ischemic stroke.” For “ischemic stroke and TIA: 50 to 325 mg [aspirin] once a day. Continue therapy indefinitely.” FDA, Federal Register. 1998.63:56802–56819.](https://image.slidesharecdn.com/3510s102albers-1233910048505471-1/85/Stroke-clinical-overview-Stroke-clinical-overview-14-320.jpg)
![New Aspirin Dosing Guidelines for Secondary Stroke Prevention FDA New professional labeling for aspirin recommends 50 to 325 mg/day American College of Chest Physicians Aspirin at 50 to 325 mg/day as an initial choice American Heart Association [50–325 mg/day proposed]](https://image.slidesharecdn.com/3510s102albers-1233910048505471-1/85/Stroke-clinical-overview-Stroke-clinical-overview-15-320.jpg)
![ACCP Antiplatelet Guidelines “ Every patient who has experienced a [non-cardioembolic] stroke or TIA...should receive an antiplatelet agent.…” “ Aspirin, clopidogrel...ticlopidine..., and the combination of aspirin and dipyridamole are all acceptable options for initial therapy.” “ Clopidogrel is recommended in favor of ticlopidine because it has a lower incidence of significant adverse effects.” “ The combination of dipyridamole and aspirin b.i.d. may be more effective than clopidogrel and has a similarly favorable adverse effect profile.” Albers GW et al. Chest . 1998;114:683S–698S.](https://image.slidesharecdn.com/3510s102albers-1233910048505471-1/85/Stroke-clinical-overview-Stroke-clinical-overview-19-320.jpg)


![Stroke Community Presentation Guide[1]](https://cdn.slidesharecdn.com/ss_thumbnails/samstrokecommunitypresentationguide1-124144563676-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)