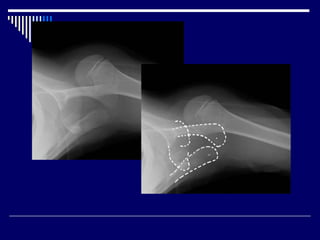
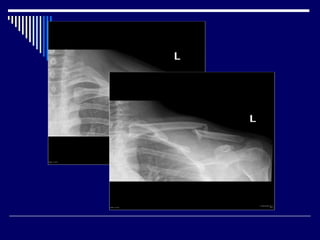
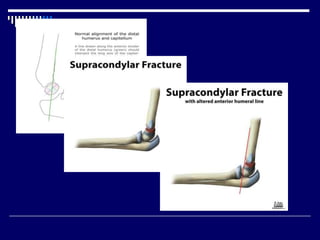
This document outlines various types of shoulder and upper arm trauma that can be seen on radiographs. It discusses shoulder dislocations, fractures of the clavicle, scapula and humerus, as well as injuries to the rotator cuff and elbow such as supracondylar fractures. For each type of injury, the document describes the typical radiographic findings and features that help with diagnosis. It provides guidance on which imaging views are necessary to properly evaluate different traumatic injuries of the shoulder girdle and upper extremity.