Downloaded 1,386 times






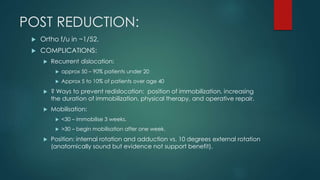
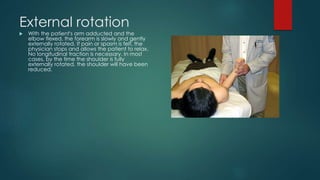

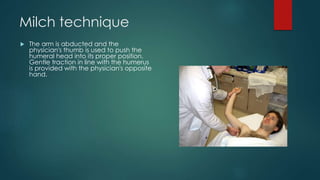

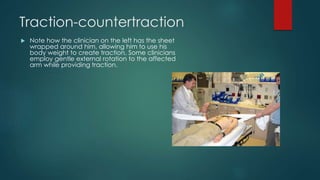

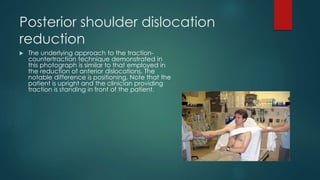


Shoulder dislocations have been documented as far back as ancient Egypt. The most common type is anterior dislocation, which accounts for 60% of cases. Reduction techniques described include external rotation, scapular manipulation, Milch, Stimson, traction-countertraction, and Spaso. Post-reduction, most patients are immobilized for 3 weeks if under 30 or begin mobilization after 1 week if over 30. Recurrent dislocation is a major complication, seen in 50-90% of patients under 20.






















































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)
