
Downloaded 62 times
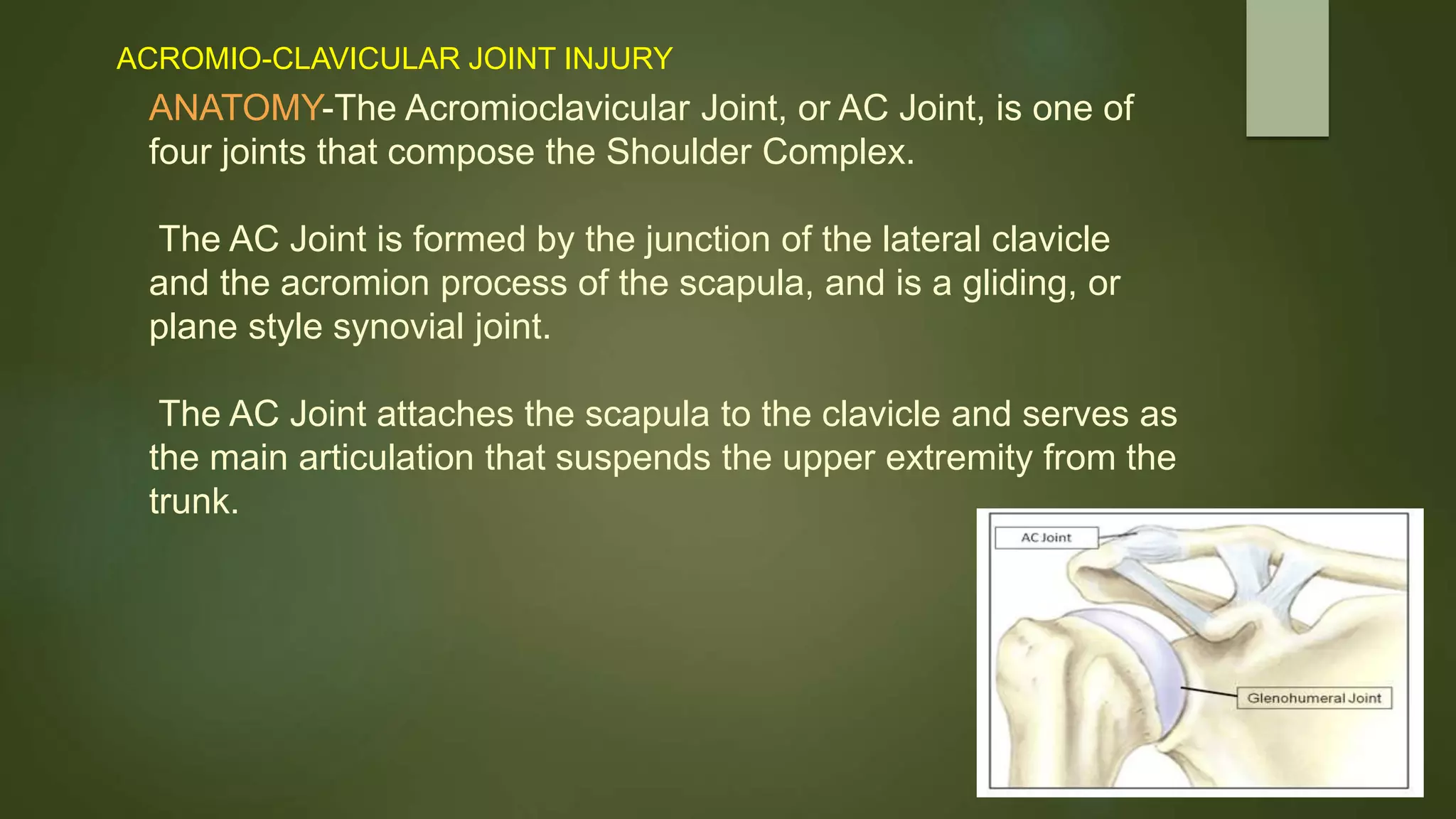


















The document discusses the anatomy and function of the acromioclavicular (AC) joint, highlighting its role in shoulder mechanics and susceptibility to injury. It categorizes AC joint injuries into traumatic and overuse types, explaining their causes, symptoms, classifications, diagnosis, and treatment options including physiotherapy. Treatment aims to relieve pain, restore joint range of motion, and strengthen the shoulder's supporting muscles.























































































