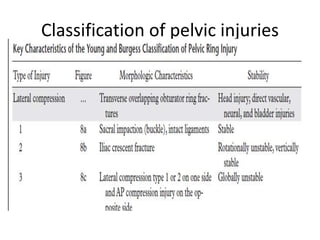
This presentation discusses injuries of the pelvis, including the anatomy, classification, and management of pelvic fractures. It notes that pelvic fractures represent 3% of skeletal injuries in the US and have a high mortality rate, especially for open fractures. Common causes are motor vehicle accidents, falls, and crush injuries. The presentation describes the Tile classification system and approaches to stabilization, hemorrhage control, and definitive fixation depending on fracture pattern and stability. Complications like DVT, ARDS, and infection are also mentioned.