Downloaded 43 times
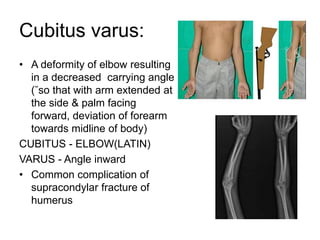
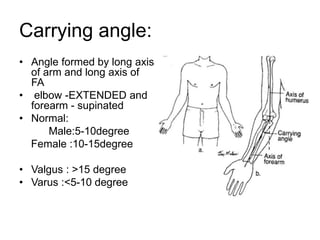
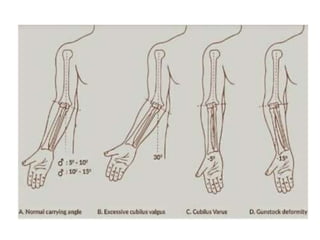
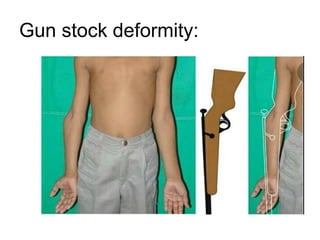

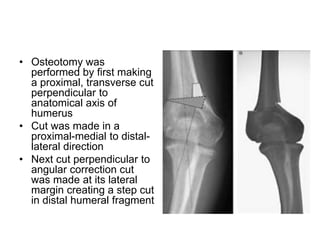

Cubitus varus is a deformity of the elbow where there is a decreased carrying angle, causing the forearm to deviate medially when extended. It is commonly caused by malunion of a supracondylar fracture of the humerus in children. Corrective options include observation with expected remodeling, hemiepiphysiodesis to alter growth, and corrective osteotomy. The French osteotomy technique involves a lateral closed wedge osteotomy held with screws or wires and remains a popular surgical approach. Complications can include stiffness, nerve injuries, recurrent deformity, nonunion and malunion.























































































