Downloaded 3,102 times
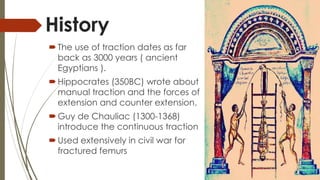
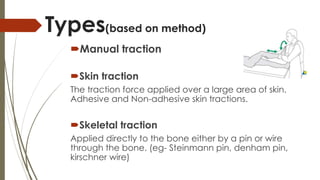
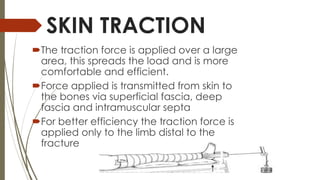


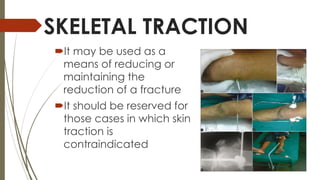
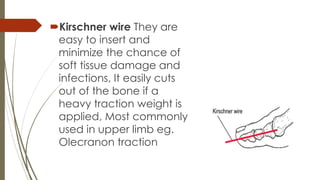


Orthopaedic traction involves applying pulling forces to parts of the body and has been used for over 100 years to treat fractures. There are several types of traction including skin traction, which applies force over a large area of skin, and skeletal traction, which applies force directly to bones using pins or wires. Traction aims to regain normal bone length and alignment, reduce fractures, and relieve pain or pressure. While it remains useful for some applications, many traction procedures have been replaced by more modern techniques.





































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)





