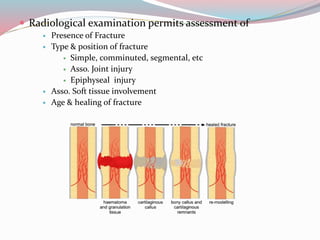
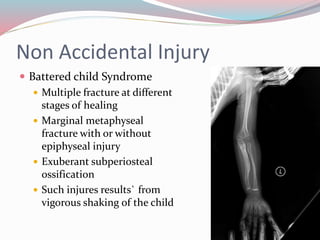
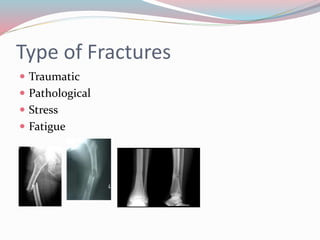
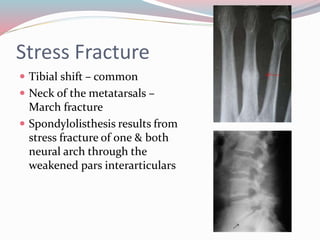
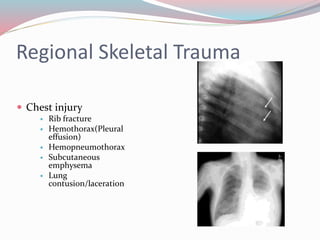
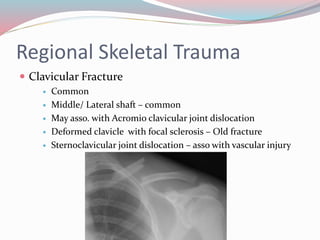
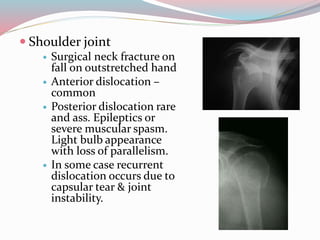
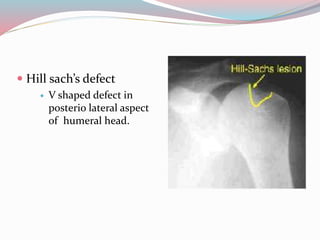
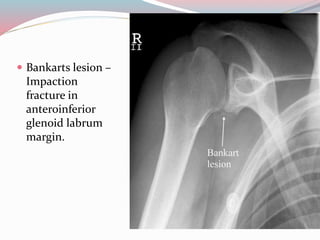
This document provides an overview of radiological examination of fractures and traumatic injuries. It discusses how radiology can be used to assess fracture type, location, complications, and associated soft tissue injuries. Specific fractures and injuries of the skull, spine, pelvis, hip, knee, ankle, shoulder and forearm are examined. Radiological signs of non-accidental injuries in children are also reviewed. The document emphasizes the importance of radiology in the diagnosis and management of skeletal trauma.