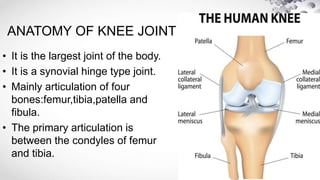
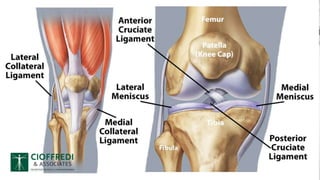
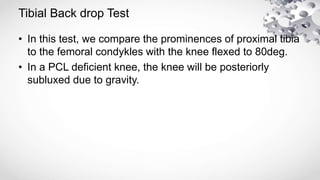
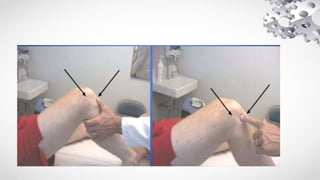
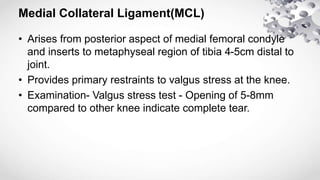
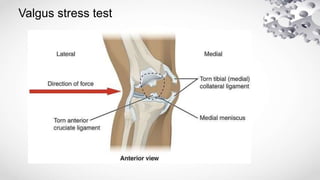
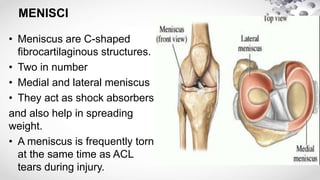
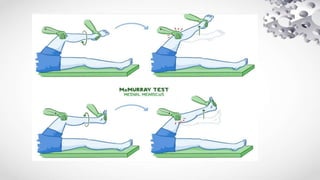
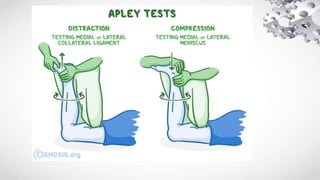
This document provides an overview of internal derangements of the knee, including injuries to ligaments and menisci. It describes the anatomy of the knee joint and the key ligaments - anterior cruciate ligament (ACL), posterior cruciate ligament (PCL), medial collateral ligament (MCL), and lateral collateral ligament (LCL). Examination techniques for each ligament are outlined. Meniscal injuries and examination tests like McMurray's test and Apley's test are also reviewed. Treatment options discussed include physical therapy, bracing, and surgical reconstruction or repair depending on the injury and individual factors.