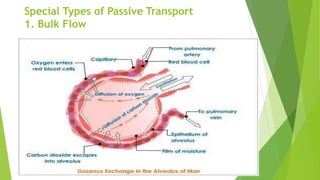
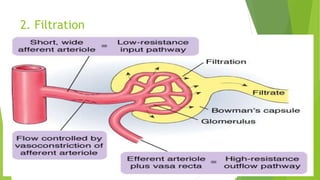
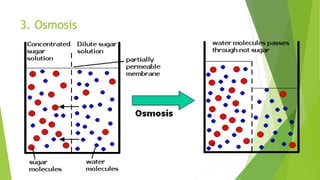
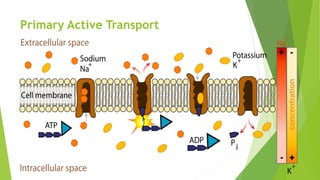
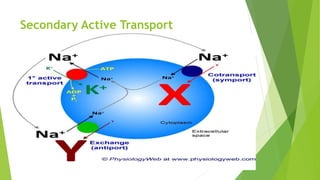
This document provides an overview of fluid and electrolyte balance and imbalance. It defines key terms related to fluids, electrolytes, and body composition. It describes the normal regulation of fluids and electrolytes in the body, including through passive and active transport mechanisms, hormones, and the sensation of thirst. It then discusses various abnormalities in fluid and electrolyte balance that can occur, including deficits, excesses, and shifts of extracellular fluid as well as various electrolyte imbalances.









![ K. Sembulingam, Prema Sembulingam. “Essentials of medical
physiology”. 5thedition (2010). Jaypee publications. Page no. 302-309
Journal of Sports medicine Volume 31, Issue 10, August 2001 ISSN:
0112-1642 (Print) 1179-2035 (Online)
Journal of Reproduction and Fertility. Supplement [1998, 53:1-14]](https://image.slidesharecdn.com/seminaronfluidandelectrolyteimbalance-150907080032-lva1-app6891/85/Seminar-on-fluid-and-electrolyte-imbalance-62-320.jpg)



![Fluid and electrolyte imbalance [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/btwa8l8ysletobnf0row-signature-f3069b4a7063ad7d39b14083d6e8689bac823dbcf19c3f5cb443fa8d754857b7-poli-171013171124-thumbnail.jpg?width=640&height=640&fit=bounds)

















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
















