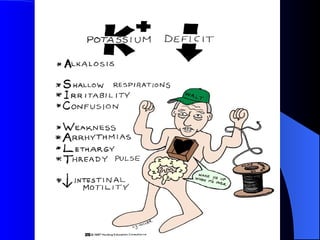
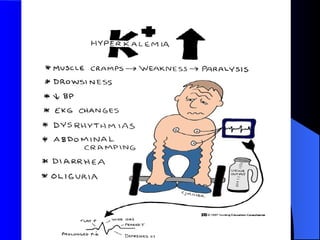
The document discusses fluid and electrolyte imbalances, including types, causes, clinical manifestations, and treatment interventions for conditions such as fluid volume deficit and excess, as well as various electrolyte imbalances like hypokalemia, hyperkalemia, hyponatremia, and hypernatremia. It provides specific assessment findings and treatment options, including dietary changes, fluid management, drug therapy, and monitoring techniques. The information is structured to aid in the understanding of clinical signs, causes, and appropriate nursing interventions.







































































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)





