Downloaded 135 times








![Fluid and electrolyte imbalance [autosaved]](https://image.slidesharecdn.com/btwa8l8ysletobnf0row-signature-f3069b4a7063ad7d39b14083d6e8689bac823dbcf19c3f5cb443fa8d754857b7-poli-171013171124/85/Fluid-and-electrolyte-imbalance-autosaved-71-320.jpg)

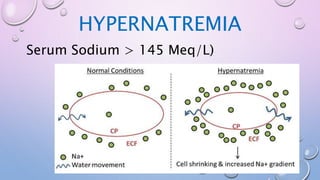
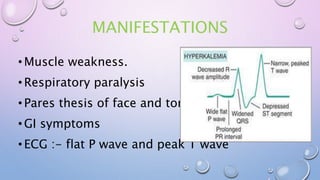
This document discusses fluid and electrolyte imbalance. It begins by explaining the importance of fluid and electrolytes in maintaining homeostasis. It then defines key terms like homeostasis, osmolality, diffusion, isotonic solutions, and active transport. The document goes on to describe different fluid imbalances like extracellular fluid volume deficit, third spacing of fluids, and intracellular fluid volume excess. It also covers various electrolyte imbalances including hypocalcemia, hypokalemia, hyperkalemia, hyponatremia, and hypernatremia. For each imbalance, it discusses etiology, clinical manifestations, laboratory findings, and treatment approaches.




















































































