Download as PPSX, PPTX

![Plasma osmolarity:
Serum Osm: 275-290 mosm/kg
Calc = 2x[Na] + [glucose]/18 + [ BUN]/2.8 +
[ethanol]/4.6](https://image.slidesharecdn.com/hyponatremia-120316120415-phpapp02/85/Hyponatremia-14-320.jpg)

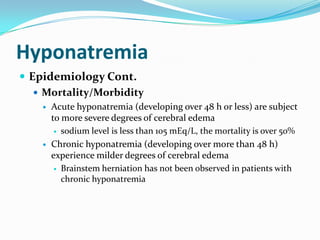
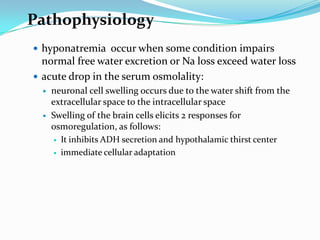
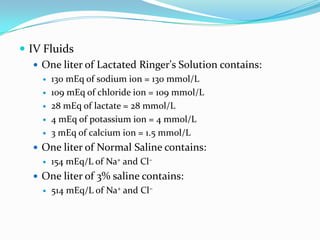
![Step-wise Approach
Serum Osm: 275-290 mosm/kg
Calc = 2x[Na] + [glucose]/18 + [ BUN]/2.8 + [ethanol]/4.6
Isotonic: PseudohypoNa
Hyperproteinemia, Hyperlipidemia
High/Hyperosmolar
hyperglycemia (1.6/100), mannitol
Low/Hypoosmolar](https://image.slidesharecdn.com/hyponatremia-120316120415-phpapp02/85/Hyponatremia-17-320.jpg)








The document discusses hyponatremia, defining it as a low serum sodium concentration and describing the physiology and pathophysiology of sodium regulation in the body. It examines the epidemiology, classification, clinical manifestations, diagnosis, and treatment of hyponatremia, providing details on evaluating volume status, calculating sodium deficits, and correcting sodium levels based on chronicity and symptoms.























































































