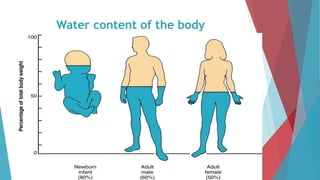
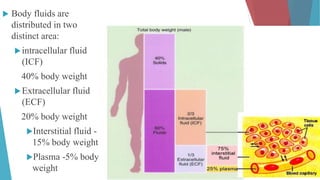
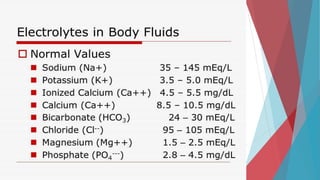
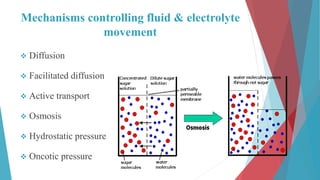
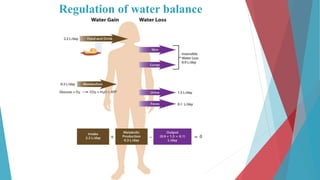
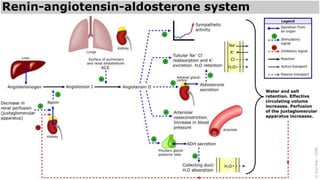
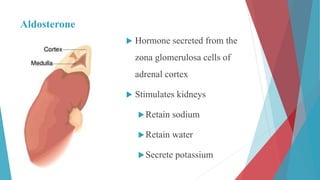
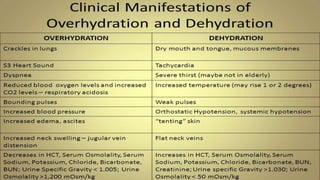
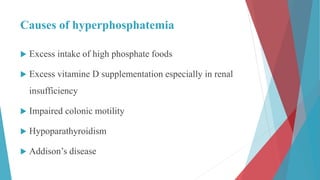
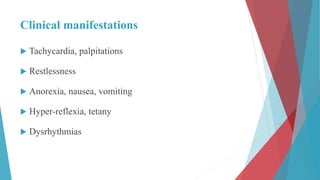
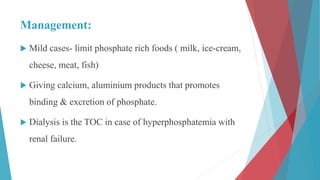
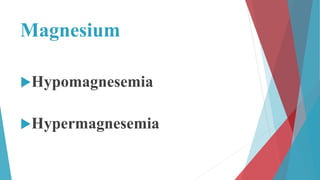
The seminar on fluid and electrolyte imbalance covers essential aspects of body fluid distribution, regulation, and the effects of imbalances such as dehydration and overhydration. Key hormones like aldosterone and antidiuretic hormone are discussed, along with conditions like hyponatremia and hypernatremia, detailing their causes, symptoms, and management strategies. Furthermore, critical management techniques for electrolyte imbalances, including nursing interventions and dietary recommendations, are essential for maintaining homeostasis.















![Fluid and electrolyte imbalance [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/btwa8l8ysletobnf0row-signature-f3069b4a7063ad7d39b14083d6e8689bac823dbcf19c3f5cb443fa8d754857b7-poli-171013171124-thumbnail.jpg?width=640&height=640&fit=bounds)
















































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)








![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)





