Downloaded 76 times

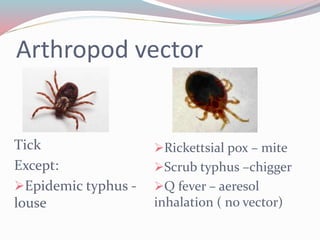


Rickettsiae are gram-negative, obligate intracellular bacteria that are transmitted to humans through arthropod vectors such as ticks, mites, lice, and chiggers. In India, rickettsial diseases are commonly found in the sub-Himalayan belt and states such as Jammu and Kashmir, Nagaland, Himachal Pradesh, Uttaranchal, Rajasthan, Assam, West Bengal, Maharashtra, Kerala, Tamil Nadu, and Delhi. Rickettsiae are classified into spotted fever group, typhus group, scrub typhus, ehrlichioses and anaplasmosis, and Q fever. Common symptoms include fever, rash, and headache





























































![RIKETTSIAL DISEASE IN INDIA [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/rikettsialdiseaseautosaved-240331142139-5d5a8fb7-thumbnail.jpg?width=640&height=640&fit=bounds)